Maternal Supplementary Folate Intake, Methylenetetrahydrofolate Reductase (MTHFR) C677T and A1298C Polymorphisms and the Risk of Orofacial Cleft in Iranian Children
-
Ebadifar, Asghar
-
Dentofacial Deformities Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
-
Kamali, Koorosh
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran
-
Khoshbakht, Tayyebeh
-
Genetic Research Centre, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
-
 Ameli, Nazila
Orthodontic Department, Dental school, Semnan University of Medical Sciences, Semnan, Iran, Tel: +98 23 33448996; E-mail: nazilaa.aameli@gmail.com
Ameli, Nazila
Orthodontic Department, Dental school, Semnan University of Medical Sciences, Semnan, Iran, Tel: +98 23 33448996; E-mail: nazilaa.aameli@gmail.com
-
Orthodontic Department, Dental school, Semnan University of Medical Sciences, Semnan, Iran
Abstract: Background: The purpose of this study was to describe the association of MTHFR gene single nucleotide polymorphisms (C677T and A1298C) and maternal supplementary folate intake with orofacial clefts in the Iranian population.
Methods: In this case-control study, peripheral venous blood was taken from 65 patients with orofacial clefts and 215 unaffected controls for DNA extraction and kept in EDTA for further analysis. The genotyping was carried out using Polymerase Chain Reaction (PCR) followed by Restriction Fragment Length Polymorphism (RFLP) and gel electrophoresis. Data were analyzed using Chi square test and logistic regression tests.
Results: Genotype frequencies of 677TT were reported to be 13.5 and 36.1% in controls and CL/P patients, respectively, which showed a significant difference compared to CC as reference (OR=4.118; 95% CI=1.997-8.492; p=0.001). Conversely, 1298CC with frequencies of 10.8 and 12.7% in controls and patients, respectively, showed no significant difference compared to AA (OR=2.359; 95% CI=0.792-7.023; p=0.123). Comparing patients whose mothers did not report the folate supplement intake during pregnancy, to controls, it was observed that lack of folate intake was a predisposing factor for having a child with oral clefts (OR=5/718, p=0.000).
Conclusion: Children carrying the 677TT variant of the MTHFR gene may have an increased risk of CL/P. In addition, the finding that the risk associated with this allele was obviously higher when the mothers didn't use folic acid, supports the hypothesis that folic acid may play a role in the etiology of CL/P.
Introduction :
Cleft lip with or without cleft palate (CL/P) is among the most common orofacial congenital anomalies in the world 1. Several epidemiological studies have reported the prevalence of cleft lip and/or palate in Iran and worldwide 2-8. Nonsyndromic CL/P (nsCL/ P) follows a multifactorial inheritance pattern in which both environmental and genetic factors are considered to play a significant role 9.
Determining the genetic risk factors of CL/P has been the subject of numerous studies 10. Also, it has been claimed that environmental factors such as maternal folic acid intake affect the risk of orofacial clefts in some pregnancies, thus, it might be hypothesized that variants of genes involved in folic acid metabolism pathway, could be associated with the risk 9,11. Among genes taking part in folate metabolism, the methylenetetrahydrofolate reductase gene (MTHFR) has been the most frequent one which is associated with nsCL/P 12-14.
It produces an enzyme which catalyzes the methylation of homocysteine amino acid to methionine. Any defect on this pathway can result in methionine deficiency and the accumulation of homocysteine. In addition to critical role of methionine as an important precursor in the DNA and RNA methylation process, high serum homocysteine levels are teratogenic during the embryogenesis 15,16.
Within the MTHFR gene, two common polymorphisms, (C---T) and (A---C), exist at positions 677 and 1298, respectively 17. Several associations have been reported between the polymorphisms in the MTHFR gene and the risk of nsCL/P 12-14. However, results have been contradictory as in a study conducted by Han et al. It was shown that A1298C polymorphism would have a protective role rather than being a predisposing factor for cleft lip and palate 18.
Numerous studies evaluated the relationship between MTHFR gene polymorphisms and nsCL/P but none of them examined Iranian patients. As a comprehensive genetic study on CL/P, a case-control study of the MTHFR polymorphisms was performed. The main objective of the present study was to determine the association between nsCL/P and C677T, A1298C polymorphisms in the MTHFR gene and the role of maternal supplementary folate intake as a risk factor for nonsyndromic orofacial clefts.
Materials and Methods :
In this study, 65 patients with nonsyndromic CL/P (isolated CL/P without any other organ disorders) and 215 unaffected controls were included which were matched to cases regarding age, gender and socio-economic status. Patients with other facial or skeletal malformations, metabolic or neurologic disorders or anomalies of other organ systems were excluded. Samples were recruited from Mofid Hospital in Tehran, Iran in 2012-2013. Ethical approval for the study was obtained from the Ethics Committee of the Dental Research Center in Shahid Beheshti University for dentofacial deformities. Informed consent was obtained from all parents.
Questions on family members were intended to find other affected family members or possible minimal variants of orofacial clefts among relatives. In order to identify any possible prenatal contributory teratogenic factor that might have influenced the development of CL/P, a detailed questionnaire was applied. The questionnaire was modeled on the Centers for Disease Control (CDC) questionnaire for risk factor surveillance for birth defects (www.cdc.gov/surveillanceepractice/a_ z.html). All mothers were questioned for maternal illnesses, medication intake, history of abortion, history of cardiovascular diseases, and smoking. In this way, confounding factors associated with orofacial clefts could be limited. Control children whose mothers reported positive history of mentioned factors were excluded. In addition, the history of folate intake during the periconceptional period (ranging from 3 months prior to 1 month after conception) was evaluated through questionnaire among mothers of cases.
Peripheral venous blood was taken for DNA extraction from all affected individuals and controls.
Genotype analysis: Blood samples were collected in tubes containing 200 μl of 0.5 M EDTA and stored at -80°C until further analysis. Genotyping for C677T and A1298C gene mutations were performed by enzymatic restriction digestion of PCR products with Hinf I and MboII enzymes, respectively 19,20.
For screening the 677C---T and 1298A---C variants in the MTHFR gene, exons 4 and 7 of the gene were amplified by Polymerase Chain Reaction (PCR) following standard conditions and with the use of modified primers (4F:5'-TCTTCATCCCTCGCCTTGAA C3'; 4R: 5' -AGGACGGTGCGGTGAGAGTG-3') and (7F: 5'- CTTCTACCTGAAGAGCAAGTC -3' 7R: 5'- CATGTCCACAGCATGGAG -3'), respectively. DNA fragments were separated and visualized by electrophoresis using 8% polyacrylamide gels (Figures 1 and 2).
Statistical methods: Statistical analyses were performed using SPSS 11.5 software and data were shown as the allele frequencies and percentages. Chi square test was used to determine the difference in the genotype and gene frequency. Odds Ratios (OR) with 95% Confidence Interval (CI) were calculated from logistic regression models. P<0.05 was considered to indicate a statistically significant result.
Results :
There were three genotypes for each variant (CC, CT and TT for C677T and AA, CC and AC for A1298C), in MTHFR gene in the two groups. Table 1 shows that compared to the CC genotype, the TT genotype was significantly correlated with an increased risk of CL/P (OR=4.1; 95% CI=2-8.5; p<0.001) while comparing to the AA genotype, the CC genotype did not show a significant difference (OR=2.4; 95% CI=0.8-7; p=0.123).
According to table 2, the frequencies of the C and T alleles of C677T and A and C alleles of A1298C were 69.7%, 30.3%, 62.9% and 37.1% in the control group, respectively and 49.1%, 50.9%, 63.1% and 36.9% in the CL/P group, respectively.
Moreover, the cases were divided into two separate groups according to maternal folate intake history. Group 1 included CL/P children whose mothers had reported folate supplement intake in the questionnaire (n=23, 37.1% in C677T and n=26, 40% in A1298C) which is shown in table 3, and group 2 included affected children whose mothers did not mention folate supplement intake (n=39, 62.9% in C677T and n=39, 60% in A1298C) (Table 4).
According to table 4, compared to the CC genotype, the TT genotype was significantly correlated with an increased risk of CL/P in group 2 and this correlation was greater than the amount found in Table 1 for all of the patients compared to controls (OR=5.7 vs. OR=4.1), while this correlation was not significant according to A1298C genotypes. This finding supports the preventive effect of folate intake even in those with predisposing genotype.
Discussion :
MTHFR is one of the major enzymes in the metabolism of folic acid which catalyzes the irreversible reduction of 5, 10- methylenetetrahydrofolate to 5- methylenetetrahydrofolate 21. A change of C to T at nucleotide 677 and A to C at nucleotide 1298 in MTHFR C677T and A1298C, results in an amino acid sequence change of an alanine to valine and glutamine to alanine, respectively. Mutant protein has reduced enzyme activity which leads to DNA hypomethylation and may induce genomic instability, thereby affecting the expression of oncogenes or tumor suppressor genes 22. Several studies have been conducted to determine the association between the two functional polymorphisms (C677T and A1298C) in MTHFR gene and an increased risk of CL/P 23,24. However, the results are inconsistent due to differences in the studied populations, various genetic backgrounds and different exposures to diverse environmental risk factors, as discussed in detail below.
The results from the present study suggest that there is an association between the MTHFR C667T mutation and CL/P incidence while the correlation between A198C polymorphism and oral clefts is not supported. Several previous studies presented that the T allele of the MTHFR C677T polymorphism might be involved in the development of CL/Ps. Similar to our results, Wan et al found that the genetic polymorphism of MTHFR C677T is associated with the development of nonsyndromic cleft lip and palate in Chinese population 25.
Also, a meta-analysis demonstrated that among Asians, CT heterozygote, TT homozygote and CT/TT of infants' MTHFR C677T variant could contribute to elevated risk of nonsyndromic orofacial clefts, compared with CC wild-type homozygote (OR=1.74 for CT vs. CC, OR=2.3 for TT vs. CC and OR=1.74 for CT/TT vs. CC) 12.
In addition, comparable studies could not show any association between the C677T polymorphism and CL/ P. Several explanations might be responsible for these discrepant findings. For neural tube defects (NTD), it has been claimed that MTHFR C677T polymorphism may only be a risk factor in populations with poor folate nutrition but under condition of complete folate status, potential association may be masked. Similarly, the MTHFR 677T risk allele may only have a significant role in the etiology of nonsyndromic CL/Ps under the conditions of overall folate deficiency 10.
Several studies have shown no significant relationship between A1298C polymorphism and oral clefts. In a study by Jagomagi et al, it was reported that A1298C polymorphism is not directly connected to the risk of developing CL/P 10. Moreover, many studies have shown similar results 13,14.
Conversely, in several studies, a protective role of A1298C polymorphism has been reported 12,18. Han et al in a study of Chinese patients demonstrated that 1298AC and CC genotype frequencies were significantly greater in control group compared to CL/P patients, emphasizing the protective role of this polymorphism 18.
In this study, an inverse association was found between positive history of maternal folate intake and CL/P in children, which could be representative of preventive role of acid folic. The results of previous studies have been inconsistent. Kelly et al reported that taking folic acid might partially prevent cleft lip and palate 26. In a study of gene-environment interaction between the MTHFR C677T polymorphism and folic acid in the etiology of orofacial clefts, Butali et al demonstrated a reduced risk of CL/P with maternal folic acid use (OR=0.7, p=0.008) and with supplements containing folic acid (OR=0.8, p=0.028) 27. These findings could be explained by the critical role of folic acid on the prevention of recurrence and occurrence of neural tube defects 28.
Conversely, in a study of all types of clefts in the U.K, Little et al observed that the maternal serum or plasma folate levels do not have any association with CL/P in children 29. This finding may point to the possible complexity of etiologically associated factors. Munger et al, using the L. casei assay in the Philippines, found that the mean red cell folate level of mothers of CL/P cases was significantly higher than that in control mothers in the two geographic areas 30. However, a complicating issue may be differences in the method used to assess maternal folate status.
The lack of supplementary folate intake found to be associated with increased risk of oral clefts in this study, can be corrected by folic acid, even in relatively small doses. Thus, our study shows the importance of educating people regarding the critical role of folic acid supplements in reducing oral clefts.
Conclusion :
In conclusion, it was found that children carrying the 677TT variant of the MTHFR gene may have an increased risk of CL/P. In addition, the finding that the risk associated with this allele was obviously higher when the mothers did not use folic acid, supports the hypothesis that folic acid may play a role in the etiology of CL/P. However, studies of various designs with larger sample sizes and different methods of measuring vitamin consumption are suggested to clarify the role of MTHFR in orofacial clefts.
Acknowledgement :
This study is the result of the research performed by Dr. Nazila Ameli for her post-graduate degree in Orthodontics under Dr. Ebadifar supervision. We would like to thank Dr Rozrokh (Head of Mofid Hospital), Mofid Hospital staff (Mrs Asgari and Mrs Safavi) and Genetic Research Center (Ms Moghadam) for their kind help in recruiting study subjects and contributions in the genetic analysis. Moreover, the research was granted by Dentofacial Deformities Research Center, Research Institute of Dental Sciences, Shahid Behehsti University of Medical Sciences, Tehran, Iran.
Conflict of Interest :
None declared.
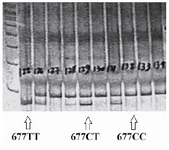
Figure 1. PCR-RFLP pattern of MTHFR C677T polymorphism di-gested with Hinf1 restriction enzyme.
|
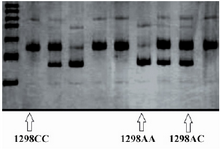
Figure 2. PCR-RFLP pattern of MTHFR A1298C polymorphism di-gested with Mbo II restriction enzyme.
|
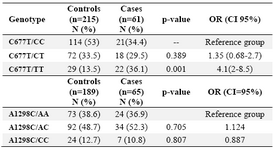
Table 1. MTHFR C677T and A1298C genotype frequencies and the CL/P risk
(CI= Confidence Interval, N= Number, OR= Odds Ratio)
|
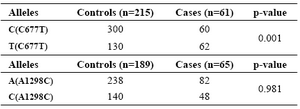
Table 2. MTHFR C677T and A1298C allele frequencies between two groups
|
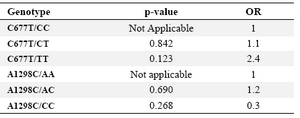
Table 3. MTHFR C677T and A1298C genotypes and the risk of CL/P in cases with positive history of maternal folate intake
(OR= Odds Ratio)
|
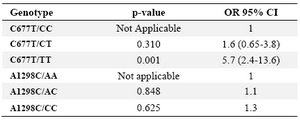
Table 4. MTHFR C677T and A1298C genotypes and the risk of CL/P in cases with negative history of maternal folate intake
(OR= Odds Ratio)
|
|