Artificial Intelligence-Assisted CRISPR Gene Editing: Current Advances, Clinical Challenges, and Future Directions in Precision Medicine
-
 Yousefian, Mahdi
Department of Advanced Technologies, TeMS.C., Islamic Azad University, Tehran, Iran, Tel: +98 9208008695; Fax: +98 21 76226989; E-mail: Yousefian.Mahdi2004@gmail.com
Yousefian, Mahdi
Department of Advanced Technologies, TeMS.C., Islamic Azad University, Tehran, Iran, Tel: +98 9208008695; Fax: +98 21 76226989; E-mail: Yousefian.Mahdi2004@gmail.com
-
Baharmast, Maryam
-
Department of Advanced Technologies, TeMS.C., Islamic Azad University, Tehran, Iran
Abstract: Recent advances in Artificial Intelligence (AI) have profoundly transformed the field of genome editing, particularly through integration with the Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR) technology. This review highlights how AI-driven computational models are reshaping guide RNA (gRNA) design, off-target prediction, and editing precision in CRISPR–Cas systems. A PRISMA-informed literature survey was conducted using PubMed, Scopus, EMBASE, and Google Scholar databases to identify studies exploring AI-assisted CRISPR applications in gene therapy and biomedical research. The results demonstrate that deep learning, machine learning, and reinforcement learning approaches significantly enhance prediction accuracy, algorithmic efficiency, and translational potential across genetic diseases such as β-thalassemia, muscular dystrophy, and cancer. Moreover, ethical challenges, algorithmic bias, and data security concerns remain critical barriers to clinical adoption. This review also discusses the emerging landscape of AI-assisted CRISPR research in Iran, emphasizing national progress, infrastructural constraints, and future opportunities. Overall, the convergence of AI and CRISPR technologies promises to advance precision medicine by accelerating the development of personalized, efficient, and ethically responsible genome-editing solutions.
Introduction :
Over the past decade, genome editing has emerged as one of the most transformative innovations in modern biology and medicine. Among genome editing tools, the Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR) and CRISPR-associated (Cas) systems have become the gold standard, offering simplicity, flexibility, and efficiency compared to earlier methods such as Zinc-Finger Nucleases (ZFNs) and Transcription Activator-Like Effector Nucleases (TALENs).
Since the landmark discovery of CRISPR–Cas9 as a programmable nuclease in 2012, this technology has expanded rapidly across research and medicine, pro-viding new possibilities for precise gene correction and therapeutic intervention. Clinical studies have demonstrated encouraging results in diseases such as sickle cell disease and β-thalassemia, where ex vivo edited hematopoietic stem cells have achieved long-term correction of genetic defects.
Similar approaches are being explored for muscular dystrophies, hereditary blindness, and immunotherapy, highlighting the broad therapeutic potential of CRISPR- based editing. However, despite remarkable success in preclinical and early clinical studies, CRISPR still faces limitations that hinder its full therapeutic translation. Major challenges remain, including off-target activity, variable efficiency across cell types, and delivery difficulties in vivo. Off-target effects can lead to unwanted mutations or chromosomal rearrangements, posing safety concerns in therapeutic settings. To address these limitations, researchers are increasingly integrating computational intelligence to enhance guide RNA design, predict off-target risk, and optimize Cas variants.
Artificial Intelligence (AI), particularly Machine Learning (ML) and Deep Learning (DL), has transformed the analysis of biological data by revealing patterns invisible to traditional bioinformatics. Within genome editing, AI models such as DeepCRISPR, Elevation, and CRISPR-Net can predict gRNA efficiency and minimize off-target risk by analyzing sequence and epigenomic features. These AI-driven systems have improved the precision and predictability of CRISPR editing, saving both time and experimental cost. The convergence of AI and CRISPR represents more than a combination of tools—it marks a paradigm shift in precision medicine. AI models can integrate multi-omics data (genomics, transcriptomics, epigenomics) to design patient-specific editing strategies, enabling personalized and safer therapeutic outcomes.
In countries such as Iran, where monogenic disorders including β-thalassemia and muscular dystrophies have a relatively high prevalence, the integration of AI with CRISPR offers a promising and cost-effective route toward developing locally optimized gene therapies. Early-stage national initiatives in biomedical AI and genome editing have already laid the groundwork for applying these technologies within precision medicine frameworks. For example, deep learning–based frameworks can simulate editing outcomes and prioritize optimal guide RNAs before in vitro validation, accelerating translational research. Nonetheless, challenges remain in interpretability and data quality. Many AI systems function as "black boxes", limiting trust in clinical applications, while biased datasets can reduce accuracy across diverse populations. Ethical considerations—including algorithmic bias, data privacy, and the risk of germline editing—necessitate transparent governance and international regulatory oversight.
This review provides a comprehensive synthesis of recent advances in AI-assisted CRISPR genome editing, summarizing the evolution of CRISPR technologies, computational innovations, therapeutic applications, and ethical frameworks guiding their responsible integration for off-target minimization, and the evolving regulatory and ethical frameworks governing these technologies.
Materials and Methods :
Literature search strategy
This narrative review employed a structured, PRISMA-informed literature search to maximize transparency, reproducibility, and coverage. Although not a full systematic review, methods were aligned with PRISMA to specify identification, screening, eligibility, and inclusion steps 1,2 (Table 1).
Databases and sources
We searched PubMed, Scopus, Web of Science, IEEE Xplore, EMBASE, and Google Scholar to capture biomedical and computational literature relevant to AI-assisted CRISPR. EMBASE and Google Scholar were explicitly included to broaden pharmacological/clinical coverage and cross-disciplinary capture.
Search terms and strategy
Controlled vocabulary (e.g., MeSH) and free-text terms were combined. Genome-editing terms: "CRISPR", "Cas9", "Cas12", "Cas13", "base editing", "prime editing". Computational terms: "artificial intelligence", "machine learning", "deep learning", "neural networks". Therapeutic terms: "gene therapy", "clinical application", "precision medicine", "cancer", "genetic disorders", "infectious diseases".
Representative multi-database query: ("CRISPR" OR "Cas9" OR "Cas12" OR "Cas13" OR "base editing" OR "prime editing") AND ("artificial intelligence" OR "machine learning" OR "deep learning" OR "neural networks") AND ("therapy" OR "therapeutic" OR "clinical application" OR "precision medicine"). Minor syntax adjustments were applied across databases 3.
Timeframe
January 2018 to August 2025 to capture contemporary advances in AI and CRISPR while excluding early conceptual reports with limited empirical validation 2,3.
Eligibility criteria
Inclusion: 1) peer-reviewed journal articles or full conference papers; 2) original research or systematic reviews on AI-enhanced CRISPR design/optimization/ therapeutic applications; 3) English language.
Exclusion: editorials/opinions without primary data; non-peer-reviewed preprints; studies restricted to agricultural/diagnostic uses without therapeutic transferability; duplicates.
Screening and selection
Two reviewers independently screened titles/ abstracts and assessed full texts. Discrepancies were resolved by discussion or third-reviewer adjudication.
Inter-reviewer agreement was high (Cohen’s κ >0.85).
Data extraction and synthesis
We extracted: CRISPR modality; AI method (supervised ML, DL, RL, generative); dataset type (genomic/transcriptomic/structural); outcomes (on-target activity, off-target prediction, therapeutic validation); and disease context.
Studies were synthesized into five categories: 1) CRISPR advances; 2) AI in gRNA/off-target; 3) AI–CRISPR integration; 4) therapeutic applications; 5) challenges, ethics, governance.
Final dataset
~2,350 records identified; after duplicate removal and eligibility screening, 200 studies were retained for qualitative synthesis spanning experimental, computational, and translational work.
CRISPR gene editing (Table 2)
Current advances: The CRISPR–Cas system has evolved from a bacterial immune mechanism into one of the most powerful and versatile tools for genome editing. It enables precise, efficient, and cost-effective modification of specific genetic loci, outperforming earlier technologies such as ZFNs and TALENs 1. Since the introduction of CRISPR–Cas9 as a programmable nuclease system in 2012 4, various Cas variants and novel editing modalities have been developed, broadening its applications in both research and clinical contexts 4,5.
CRISPR-Cas9
Cas9 remains the most widely used and studied nuclease, capable of introducing targeted Double-Strand Breaks (DSBs) guided by a single-guide RNA (sgRNA). DNA repair occurs through Non-Homologous End Joining (NHEJ), which often introduces indels, or Homology-Directed Repair (HDR), which enables precise gene correction or insertion 6,7. Clinical studies employing Cas9 for ex vivo editing of hematopoietic stem cells have shown therapeutic potential for β-thalassemia and sickle cell disease 8. In vivo Cas9-based therapies for hereditary blindness (Leber congenital amaurosis) have also reported promising results 3.
CRISPR-Cas12 (Cpf1)
Cas12, also known as Cpf1, offers several technical advantages over Cas9, including smaller guide RNAs, staggered DNA cuts, and broader PAM sequence compatibility 4. Cas12 enzymes are also less prone to off-target activity and are suitable for multiplex genome editing 3. Cas12-based systems have been applied in both therapeutic and diagnostic research, particularly in nucleic acid detection platforms such as DETECTR 9,10.
CRISPR-Cas13
Unlike Cas9 and Cas12, Cas13 targets RNA molecules rather than DNA, allowing temporary regulation of gene expression without permanent genomic alteration 1. This feature makes Cas13 a promising tool for treating viral and neurological diseases 3,11. Cas13-based therapies have been explored for viral infections, including SARS-CoV-2 12,13, and influenza 18,19, and for transcriptome engineering in rare genetic disorders 14.
Base editing
Base editors enable the direct conversion of one DNA base into another without inducing DSBs 15. Cytosine Base Editors (CBEs) convert C→T, while Adenine Base Editors (ABEs) convert A→G. These systems reduce cytotoxicity and minimize unwanted indels, offering safer correction of pathogenic point mutations 16. Base editing has demonstrated therapeutic promise in preclinical models of Duchenne muscular dystrophy and familial hypercholesterolemia 17,18.
Prime editing
Prime editing combines a Cas9 nickase with a reverse transcriptase and a prime editing guide RNA (pegRNA) 17,19. This system enables all twelve base substitutions and small insertions or deletions without relying on donor templates or creating DSBs 20. Despite its versatility, efficiency and delivery optimization remain key challenges for clinical translation 17.
Broader applications and limitations
Together, these CRISPR systems have transformed genome manipulation—from gene disruption to highly precise DNA and RNA editing 21-23. CRISPR technologies now extend to epigenetic regulation, transcriptional control, live-cell imaging, and genome-wide functional screening 3,24. However, challenges such as limited editing efficiency, off-target effects, immune responses, and delivery constraints still hinder widespread clinical use 16,25.
AI has emerged as a powerful ally, providing computational strategies to optimize sgRNA design, predict off-target profiles, and improve Cas protein engineering. As CRISPR modalities become more complex, AI integration will play a crucial role in guiding their clinical translation 26-28.
Artificial intelligence in genomics
The emergence of AI, particularly ML and DL, has transformed the analysis of large-scale genomic data. Traditional bioinformatics methods, which rely mainly on rule-based algorithms, often fail to capture complex, nonlinear biological relationships 29,30. AI models can uncover hidden patterns, integrate diverse multi-omics datasets, and generate predictive insights that surpass conventional analytical approaches 7,31,32. These abilities make AI an essential tool for the advancement of genome editing technologies, including CRISPR.
AI in guide RNA (gRNA) design
AI has significantly improved guide RNA (gRNA) design—the key factor determining CRISPR accuracy and efficiency 9,33. Earlier gRNA selection methods were based on limited sequence motifs or empirical scoring systems, leading to inconsistent editing outcomes 34. Modern AI-driven algorithms, trained on large CRISPR datasets, now predict gRNA activity across genomic contexts with high precision 26. Convolutional Neural Networks (CNNs) and Recurrent Neural Networks (RNNs) have been employed to capture both local sequence features and broader chromatin architecture influences 18,35. Models like DeepCRISPR and CRISPR-Net integrate sequence data, epigenomic marks, and expression profiles to enhance gRNA efficiency 7,36,37.
Off-target prediction
Off-target mutations remain a major concern in clinical CRISPR applications 6,30,38. Traditional alignment-based tools often lack the accuracy required for safety assessment 39. AI models such as Elevation and CrispAI employ supervised learning and deep learning to predict off-target cleavage sites with higher sensitivity and specificity 26,40,41. By considering chromatin accessibility and DNA methylation, these models improve prediction reliability and assist in risk reduction during experimental validation 30,42,43.
Protein engineering of Cas variants
Another major use of AI lies in the rational engineering of Cas proteins. Natural Cas enzymes are limited by PAM recognition, immunogenicity, and variable editing efficiency 13. Deep generative models and reinforcement learning frameworks have been applied to design Cas variants with enhanced specificity and performance 37. AI-guided Cas9 variants show broader PAM compatibility and lower off-target activity, expanding CRISPR’s therapeutic scope 14. These innovations not only broaden the range of genomic loci accessible to editing but also enhance the clinical applicability of CRISPR technologies.
Integration with multi-omics data
AI enables comprehensive integration of genomic, transcriptomic, epigenomic, and proteomic data to guide CRISPR applications 38,44. This integration helps link gRNA design to gene regulatory networks, allowing prediction of downstream biological effects 45. Such systems-level understanding is particularly relevant for complex diseases like cancer, where multiple molecular layers interact 5. By prioritizing therapeutic targets through data-driven prediction, AI supports patient-specific CRISPR therapy design 38 (Table 3).
Challenges in AI applications
Despite rapid progress, AI applications in genomics still face important challenges. Model performance depends heavily on the quality and diversity of training datasets 26,33. Limited representation across populations can introduce bias, reducing generalizability 46. Another key limitation is interpretability—deep models often operate as "black boxes", making it difficult to justify predictions for clinical use. In addition, training large models requires extensive computational resources, restricting accessibility for smaller research groups 47-49.
In summary, AI has reshaped genomics by improving gRNA design, off-target prediction, Cas protein engineering, and integration of multi-omics data. While some technical and ethical challenges remain, AI will undoubtedly continue to accelerate the development of safe and efficient CRISPR-based therapies in precision medicine.
Integration of AI with CRISPR
The integration of AI with CRISPR-based genome editing represents a synergistic convergence that is redefining modern biotechnology. While CRISPR offers unmatched precision in genome manipulation, AI provides computational intelligence to analyze complex biological data, predict editing outcomes, and optimize experimental design 2,26,50. Together, they create end-to-end pipelines that enhance the reliability, safety, and translational potential of gene editing.
AI-assisted guide RNA design platforms
AI-powered platforms have been incorporated directly into CRISPR pipelines to improve gRNA design efficiency and specificity. Tools such as DeepCRISPR, CRISPR-Net, Azimuth, and Elevation apply deep and ensemble learning frameworks to score potential gRNAs based on on-target and off-target predictions 9,33. These systems allow researchers to screen thousands of gRNAs in silico before experimental validation, substantially reducing time and cost.
Comparative studies have shown that AI-guided predictions outperform traditional rule-based algorithms by improving on-target precision and minimizing unintended edits 8,45,61.
Closed-loop AI–CRISPR workflows
Beyond standalone tools, AI–CRISPR integration is evolving into closed-loop frameworks. In these workflows, AI models predict optimal gRNAs or Cas variants; experimental results are then fed back into the system to refine subsequent predictions 9,27,30,45. This feedback-driven cycle continuously improves both computational models and laboratory outcomes. Such adaptive pipelines are particularly valuable in preclinical settings, where rapid optimization is critical to success.
AI-guided Cas protein engineering
AI has become a key enabler in engineering novel Cas proteins with enhanced characteristics. Techniques including Generative Adversarial Networks (GANs), reinforcement learning, and structure-informed deep learning models are used to design Cas variants with broader PAM recognition, reduced immunogenicity, and higher efficiency 13,14,40,62. These improvements extend CRISPR applicability to genomic regions previously inaccessible to conventional Cas9 systems. AI-driven protein design is now a cornerstone for next-generation genome editors 9,15,37.
Therapeutic target discovery and prioritization
Another major application involves AI-assisted target prioritization for CRISPR-based therapeutics. AI models analyze large-scale multi-omics and clinical data to identify genes most critical to disease pathogenesis 5,6. These predictions are validated experimentally using genome-wide CRISPR screens, accelerating the discovery of potential therapeutic targets 4,7,26,33. Such integration between computational prediction and gene-editing validation bridges the gap between data analysis and clinical translation.
Predictive modeling of outcomes
AI-enhanced CRISPR pipelines now include predictive modeling to assess safety, efficacy, and patient-specific outcomes. By combining genomic, transcriptomic, and epigenomic data, AI models simulate editing responses and identify potential immune or off-target risks before experimentation 30,63. This approach enables precision prediction, allowing clinicians to design personalized CRISPR therapies tailored to individual molecular profiles.
Challenges in integration
Despite its promise, AI–CRISPR integration faces significant challenges. Model performance remains dependent on the availability of large, high-quality datasets, which are often limited or biased toward specific organisms or cell types 64. Generalization across tissues and species remains uncertain, and the “black-box” nature of deep models limits interpretability and clinical trust 65. To address these barriers, ongoing efforts focus on developing explainable AI (XAI) systems, expanding open genomic datasets, and fostering interdisciplinary collaboration between computer scientists and biologists 66. In summary, the convergence of AI and CRISPR forms a self-improving ecosystem—enhancing guide RNA design, protein engineering, target prioritization, and predictive modeling. This synergy not only accelerates therapeutic innovation but also lays the foundation for the next generation of precision gene editing.
Therapeutic applications of AI-assisted CRISPR
The convergence of AI and CRISPR genome editing has accelerated the development of next-generation therapeutics across a broad spectrum of diseases. By enhancing guide RNA (gRNA) optimization, improving off-target prediction, and enabling patient-specific therapeutic design, AI-assisted CRISPR is paving the way for more effective and safer gene-based interventions (Tables 4-6).
Genetic disorders
Monogenic diseases, caused by single-gene mutations, are among the most promising targets for AI-enhanced CRISPR therapies. Disorders such as Sickle Cell Disease (SCD), β-thalassemia, Duchenne Muscular Dystrophy (DMD), and spinal muscular atrophy (SMA) have well-defined genetic causes, making them ideal for precise gene correction. Clinical trials using CRISPR-Cas9 for ex vivo Hematopoietic Stem Cell (HSC) editing have already shown durable therapeutic efficacy in SCD and β-thalassemia patients 19. AI tools further refine these applications by optimizing gRNA sequences, minimizing off-target risks, and tailoring editing strategies to individual genotypes 11,19,25,67. In DMD, for example, AI-driven base editing systems have achieved higher correction accuracy in preclinical models 15,68.
Cancer
CRISPR has become a transformative technology in cancer research and therapy, particularly for engineering immune cells such as CAR-T and TCR-T cells 69,70. These therapies depend on precise genome editing to enhance T-cell tumor recognition and cytotoxicity. AI models improve this process by predicting optimal gRNAs and minimizing oncogenic off-target risks 4,23. In addition, AI-based analysis of large-scale cancer genomics datasets can identify novel oncogenes and synthetic lethal gene pairs, which are subsequently validated through CRISPR functional screens 5-7,71. This combined pipeline accelerates the discovery of personalized immunotherapies and molecularly targeted treatments 17,72.
Infectious diseases
AI-assisted CRISPR tools hold great potential for antiviral therapy. The RNA-targeting capability of Cas13, when combined with AI-guided sequence optimization, enables rapid identification of conserved viral RNA motifs suitable for disruption 9,73. For instance, during the COVID-19 pandemic, AI-enhanced CRISPR-Cas13 systems were designed to target key regions of the SARS-CoV-2 genome within weeks 16,39,74. Similar approaches are being explored for HIV to eradicate latent viral reservoirs and for influenza to target conserved genes across viral strains 11,20,36,75,76. AI dramatically reduces the time required to adapt CRISPR antivirals to emerging pathogens, improving global pandemic preparedness.
Neurological and neurodegenerative disorders
Gene editing in the Central Nervous System (CNS) faces unique challenges due to limited delivery and the Blood–Brain Barrier (BBB). However, AI-assisted CRISPR is opening new possibilities for disorders such as Huntington’s disease, Amyotrophic Lateral Sclerosis (ALS), and Rett syndrome 24,63. By integrating genomic, transcriptomic, and epigenomic data, AI models can identify neuron-specific therapeutic targets and predict off-target activity in neural tissues 27,30. Preclinical studies have already demonstrated that CRISPR-mediated silencing of mutant huntingtin alleles can alleviate disease phenotypes, and AI tools are expected to further refine these interventions 16,76,77.
Toward personalized medicine
Perhaps the most transformative contribution of AI-assisted CRISPR lies in advancing personalized medicine. By combining genomic, epigenomic, and transcriptomic data from individual patients, AI can design tailored CRISPR systems optimized for each person’s molecular profile 78,79. Such personalization not only improves efficacy but also reduces risks associated with inter-patient variability in genetic backgrounds. The long-term vision involves AI analyzing a patient’s data to design and simulate CRISPR interventions in silico, predicting outcomes and safety before treatment 19,79,80. This represents a paradigm shift from generalized therapies toward individualized, precision gene editing.
Summary
Across genetic, oncological, infectious, neurological, and rare diseases, AI-assisted CRISPR is transforming the landscape of therapeutic development. Its combined computational and molecular strengths enable innovations that are both effective and safe. While challenges remain in delivery, regulation, and ethics, the integration of AI with CRISPR continues to drive the field toward fully personalized and predictive medicine.
Challenges and ethical considerations
Despite its revolutionary potential, the integration of AI and CRISPR genome editing faces significant technical, clinical, and ethical challenges that must be addressed to ensure safe and equitable implementation 11,30,31,81 (Table 7).
Technical challenges
One of the most critical issues is the persistent risk of off-target effects. Even with AI-enhanced gRNA design, current models cannot fully prevent unintended genomic alterations 26,62. Such edits may disrupt essential genes, activate oncogenes, or cause chromosomal rearrangements with serious biological consequences 41,63. Another technical limitation is the dependence of AI models on data quality. Most available datasets are derived from limited cell lines or populations, which restricts model generalizability 46. Moreover, the "black-box" nature of deep learning algorithms limits interpretability and regulatory confidence 40,82. Computational cost is another obstacle, as large-scale AI training requires substantial resources, often inaccessible to smaller research centers 50.
Clinical challenges
Delivery remains the major bottleneck for CRISPR-based therapeutics. Efficient and safe delivery of Cas proteins and gRNAs to target tissues remains challenging 80,83,84. While viral vectors (e.g., AAV, lentivirus) provide high transduction efficiency, they raise immunogenicity and insertional mutagenesis concerns 4. Non-viral systems, including lipid nanoparticles and polymeric carriers, show promise but still require optimization for consistent therapeutic outcomes 85. Furthermore, the regulatory landscape for AI–CRISPR systems remains underdeveloped. Existing frameworks were not designed to evaluate hybrid computational–biological technologies, creating uncertainty in validation and approval processes 23. High cost and scalability challenges may limit accessibility, especially in resource-limited settings, raising issues of equity in healthcare delivery 86.
Ethical considerations
The combination of AI and CRISPR raises complex ethical and societal issues that extend beyond laboratory safety. Algorithmic bias is one concern: if AI models are trained primarily on genomic data from specific populations, they may yield less accurate results for underrepresented groups 87,88. This could exacerbate existing global health disparities. This could exacerbate global health disparities and ethical inequalities.
Another major concern is data privacy
AI-assisted CRISPR relies on vast amounts of genomic and clinical data, raising questions about confidentiality, informed consent, and potential misuse 39,88. Secure data governance and encryption frameworks, including federated learning and blockchain-based audit trails, are essential to mitigate these risks. Perhaps the most debated issue involves human germline editing. While AI can enhance precision and reduce errors, it may also lower the barriers to heritable genetic modification 79,87,89. Although germline editing could theoretically prevent severe genetic diseases, it raises unresolved questions about consent for future generations and ethical limits of human enhancement 67,90.
Governance and global equity
Addressing these challenges requires transparent governance, global collaboration, and public engagement. Regulatory agencies must adapt to evaluate AI-informed biological systems with new standards for safety, explanation, and accountability 67,91. Equitable access must also be ensured so that AI–CRISPR therapies do not remain confined to wealthy nations or privileged populations 92,93. Interdisciplinary cooperation among scientists, ethicists, policymakers, and patient communities is vital to shape the responsible trajectory of this technology.
AI-assisted CRISPR research in Iran
Progress, constraints, and future prospects: Over the past decade, Iran has witnessed remarkable growth in biomedical sciences, particularly in genetics, stem cell biology, and biotechnology. National institutes such as the Royan Institute, Pasteur Institute of Iran, Tehran University of Medical Sciences, and Sharif University of Technology have laid the foundation for genomic and bioinformatics research that supports emerging genome-editing technologies.
Within this framework, several Iranian research groups have begun to explore the integration of artificial intelligence (AI) into CRISPR–Cas systems. Early efforts have focused on optimizing guide RNA (gRNA) design, identifying disease-specific targets, and predicting off-target risks in conditions of national importance such as β-thalassemia, breast cancer, and certain metabolic disorders.
Despite these promising developments, multiple challenges remain. Limited access to large annotated genomic datasets and high-performance computing infrastructure restricts the scalability of AI-driven CRISPR modeling in Iran. Moreover, the gap between computational research and experimental validation slows the pace of translational outcomes. Nevertheless, the increasing number of interdisciplinary collaborations, government-supported precision medicine initiatives, and the expansion of bioinformatics graduate programs suggest that Iran is moving toward building a sustainable ecosystem for AI-assisted genome editing.
Looking ahead, investment in open genomic databases, ethical data-sharing policies, and cross-institutional partnerships with international consortia could significantly accelerate Iran’s contribution to the global landscape of AI-enabled gene editing.
Summary
In summary, AI-assisted CRISPR technologies face challenges that extend beyond technical optimization. Their future success depends on ethical responsibility, clinical validation, and global inclusivity. A proactive and transparent governance approach is essential to ensure that AI–CRISPR integration advances human health while avoiding new forms of inequality or ethical misuse.
Future directions
The convergence of artificial intelligence (AI) and CRISPR genome editing remains in its early stages, yet the rapid pace of innovation suggests a transformative future for precision medicine and biotechnology 29, 94. To ensure sustainable progress, upcoming research must focus on transparency, personalization, novel modalities, and responsible governance.
Explainable and transparent AI
One urgent priority is developing explainable AI (XAI) models to enhance interpretability. Most current deep learning algorithms function as "black boxes", limiting clinical confidence and regulatory approval 25,29,47,50. Future systems should not only predict gRNA performance or off-target risk but also clarify the reasoning behind each prediction, enabling reproducibility and informed clinical use 95,96.
Personalized and precision editing
Integration of multi-omics data—genomics, transcriptomics, epigenomics, and proteomics—will drive the next wave of personalized CRISPR therapies. AI models will design patient-specific gRNAs and Cas variants optimized for each individual’s genome, disease subtype, and predicted therapeutic response 13, 14.
As sequencing costs decrease, AI-guided personalization will transition from concept to clinical reality, supporting tailored gene editing for genetic and complex diseases.
Expansion of editing modalities
CRISPR is rapidly evolving beyond Cas9: AI will accelerate the discovery and engineering of next-generation nucleases, including Cas12, Cas13, base editors, and prime editors 24,65. Reinforcement learning and generative protein design will help create Cas variants with broader PAM recognition, higher fidelity, and lower immunogenicity. AI will also optimize epigenetic editing and synthetic gene circuits, expanding CRISPR’s therapeutic scope 22,74.
Integration with emerging technologies
Future AI–CRISPR applications will merge with other disruptive technologies, such as nanotechnology, organoids, and lab-on-a-chip systems. AI can guide nanoparticle design for precise tissue targeting and evaluate CRISPR efficacy in organoid-based disease models 45,47. In combination with single-cell multi-omics, AI will predict editing outcomes at unprecedented resolution, enabling safer and more predictable interventions 22.
Predictive and preventive genomics
The long-term vision of AI-assisted CRISPR extends from therapy to disease prevention. By forecasting genetic predispositions and modeling early interventions, AI may help design prophylactic gene edits to prevent disease onset 92,95. Although ethically sensitive, this proactive approach could shift medicine from treatment-based to preventive and truly personalized care.
Ethical and global governance outlook
As technology advances, governance must evolve in parallel. International cooperation is essential for developing shared standards on data transparency, algorithmic fairness, and equitable access 79. A global ethical framework should define clear boundaries for acceptable applications and prevent misuse—such as unauthorized germline editing—while promoting innovation. Broad engagement among scientists, policymakers, ethicists, and the public will be necessary to sustain ethical progress.
Establishing regional AI–CRISPR research networks in scientifically emerging countries such as Iran can help bridge the global divide in access to computational resources and genomic data. Such collaborations would enhance algorithmic transparency, facilitate ethical data governance, and promote equitable participation in the rapidly evolving field of precision genome editing.
Summary
The next decade of AI-assisted CRISPR will be defined by explainable algorithms, personalized therapeutics, novel Cas systems, nanotech integration, and preventive genomics. If developed responsibly, this convergence will not only revolutionize genetic medicine but also redefine the boundaries of human health and bioethics.
Conclusion :
The integration of AI with CRISPR genome editing marks a paradigm shift in biotechnology and personalized medicine. CRISPR has already revolutionized genome engineering, enabling targeted correction of genetic defects, while AI amplifies its precision and scalability 30. This review highlights how AI strengthens every stage of the CRISPR workflow—from gRNA design and off-target prediction to Cas protein optimization and multi-omics integration. Together, these technologies have demonstrated transformative potential across genetic, oncological, infectious, neurological, and rare diseases, while also introducing new ethical and clinical considerations 23.
Looking ahead, responsible development of explainable AI, personalized editing strategies, and next-generation Cas variants will be critical for safe clinical adoption. Interdisciplinary collaboration among biologists, computational scientists, clinicians, ethicists, and regulators will shape whether this technology fulfills its promise or creates new inequities 21,22,39.
In conclusion, AI-assisted CRISPR represents not just an incremental step but a transformative leap toward curative and preventive medicine. When guided by transparency, ethics, and inclusivity, it has the potential to redefine the future of healthcare by addressing disease at its genetic foundation.
Data availability statement
No new datasets were generated or analyzed in this study. All data are based on previously published and cited sources.
Ethical approval statement
This study did not involve human participants and therefore did not require institutional ethics approval.
Acknowledgement :
The authors would like to express their appreciation to the Department of Advanced Technologies, Tehran Medical Sciences Campus, Islamic Azad University, Tehran, Iran, for supporting this research. This review article did not involve any studies with human participants or animals; therefore, ethical approval was not required.
Conflict of Interest :
The authors declare that they have no conflicts of interest relevant to this article.
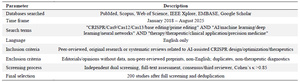
Table 1. Literature search strategy and inclusion/exclusion criteria
|

Table 2. Comparison of major CRISPR modalities – Cas9, Cas12, Cas13, base editing, prime editing
Legend: Comparative overview of major CRISPR systems highlighting mechanisms, capabilities, therapeutic uses, and limitations.
|
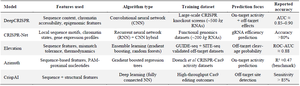
Table 3. Major AI models for gRNA design and off-target prediction
Legend: Summary of representative AI models used for gRNA design and off-target analysis, highlighting core algorithms and accuracy metrics.
|
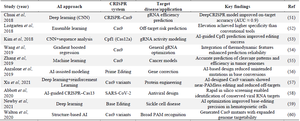
Table 4. Summary of representative studies on AI-assisted CRISPR applications
Legend: Summary of selected studies demonstrating the integration of AI techniques into CRISPR design, off-target prediction, and therapeutic translation.
An overview of key studies demonstrating the integration of Artificial Intelligence (AI) techniques into CRISPR-based genome editing workflows. Each entry summarizes the applied AI approach, CRISPR system, target disease or application, and principal findings.
Abbreviations: CNN – Convolutional Neural Network; PAM – Protospacer Adjacent Motif; AUC – Area Under the Curve.
|
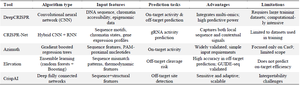
Table 5. Comparison of major AI-driven CRISPR tools
Legend: Summary of widely used AI-driven CRISPR tools, emphasizing their algorithms, strengths, and current limitations.
|
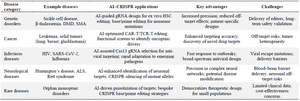
Table 6. Therapeutic applications of AI-assisted CRISPR across major disease categories
Legend: Summary of AI-assisted CRISPR applications across disease categories, highlighting therapeutic benefits and challenges.
|
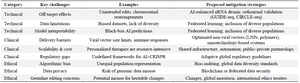
Table 7. Summary of challenges and proposed mitigation strategies
Legend: Overview of key challenges in AI-assisted CRISPR implementation with recommended mitigation strategies.
|
|