Association between PON1-rs662 Gene Polymorphism and Diabetic Retinopathy in Population of the Qom, Iran
-
Sabbaghian Bidgoli, Fateme
-
Department of Molecular and Cell Biology, Faculty of Sciences, University of Mazandaran, Babolsar, Iran
-
 Tafrihi, Majid
Department of Molecular and Cell Biology, Faculty of Science, University of Mazandaran, Babolsar, Mazandaran, Iran, Tel/Fax: +98 11 35305252, 31 55912397; E-mail: m.tafrihi@umz.ac.ir
Tafrihi, Majid
Department of Molecular and Cell Biology, Faculty of Science, University of Mazandaran, Babolsar, Mazandaran, Iran, Tel/Fax: +98 11 35305252, 31 55912397; E-mail: m.tafrihi@umz.ac.ir
-
Nakhaei Sistani, Roohollah
Department of Cell and Molecular Biology, Faculty of Chemistry, University of Kashan, Kashan, Isfahan, Iran, Tel/Fax: +98 11 35305252, 31 55912397; E-mail: r.nakhaei@kashanu.ac.ir
Abstract: Background: Diabetic retinopathy is the most severe diabetic microvascular complication that causes changes in the vessel wall. One of the genes involved in this disease is PON1, which encodes paraoxanase1 protein in liver and kidney. It might regulate inflammatory and microvascular responses to the disease. The rs662 T>C is one of the single nucleotide polymorphisms of this gene that changes glutamine to arginine at position 192.
Methods: In this study, 300 samples were collected, including 100 healthy and 100 diabetics without retinopathy, and 100 diabetics retinopathies were studied and their age range was from 30 to 80 years. Then 2.5 ml of blood was collected from all relevant individuals in tubes containing EDTANa2. This polymorphism was examined by tetra-ARMS PCR.
Results: Results showed that there is no significant correlation between genotypes and alleles related to PON1 and Diabetes (CC genotype: p=0.609; C allele: p=0.228). On the other hand, an association was observed between PON1 and diabetic retinopathy (CT+CC genotype: p<0.001; CT allele: p<0.001). Considering that the Polyphen database examined the changes caused by replacing the amino acid arginine instead of glutamine at position 129 on the protein, it does not consider these changes dangerous and has introduced this polymorphism as benign.
Conclusion: Based on the findings of this study, the rs662 locus could be considered as one of the molecular markers in future research.
Introduction :
Diabetes mellitus is the most common noncommunicable disease worldwide. It is among the leading causes of death in all socioeconomic circumstances 1. Diabetic Retinopathy (DR) is known as a major complication of diabetes mellitus, which is a leading cause of visual loss. DR is characterized by vascular abnormalities in the retina 2. Clinically, DR includes two stages: Non-Proliferative Diabetic Retinopathy (NPDR) and Proliferative Diabetic Retinopathy (PDR). NPDR is the early stage of DR. In this stage, retinal pathologies such as hemorrhages and microaneurysms are detectable. However, neovascularization occurs in PDR 3. A meta-analysis study showed that the incidence of diabetic retinopathy ranges from 22 to 127% 4. In addition, the prevalence of DR in Iranian diabetic patients is 30% 5. The pathophysiology of this disease is complex and has not been fully understood. Oxidative stress is implicated in hyperglycemia-induced abnormalities in the retina 6. In recent years, it is generally believed that genetic factors are involved in the occurrence, prevention, and treatment of DR.
Today, various polymorphisms in the promoter or coding regions have been documented in the paraoxonase 1 (PON1) gene 7. PON1, a calcium-dependent enzyme is known as a serum esterase/lactonase which is synthesized in liver 8. PON1, a polymorphic protein prevents low-density lipoprotein oxidation in diabetes 9. PON1 is an HDL-associated protein that hydrolyzes oxidized LDL-cholesterol and exerts potential atheroprotective effects 10. However, few studies reported a relationship between PON1 polymorphisms with DR. Hampe et al demonstrated that the PON1 R allele is associated with susceptibility to DR 11. Another study showed that genotype L/L was significantly associated with DR 12. Therefore, one of the polymorphisms that may play a role in DR is rs662(Q192R), and this study aimed to investigate the relationship between rs662-PON1 gene polymorphism and DR in the Qom’s population.
Materials and Methods :
Samples: In the case-control study, intravenous blood samples were collected from diabetic patients with retinopathy (n=100), without retinopathy (n=100), and healthy subjects (n=100). The inclusion criteria were age from 30 to 80 years old, and the diagnosis of retinopathy by an optometrist. All blood samples were collected from Qom hospitals in Iran from 2018 to 2022 years. This study was approved by the Ethics Committees of the Mazandaran University of Medical Science (#IR.UMZ.REC.1399.035) and all subjects signed an informed consent form before entering the study.
DNA extraction and PCR-RFLP: Genomic DNA was extracted from leukocytes of the blood samples by a standard salting out method. Extracted DNA stored at -20°C after determining the relevant concentrations and analysis on gel electrophoresis. PON1-rs662 gene polymorphisms were examined by tetra-ARMS PCR. All primers used in this research were designed by a primer design program, Oligo7 (Table 1). Each PCR reaction was performed in a final volume of 20 μl, including 100 ng of genomic DNA, 3.5 μl of 10× solution buffer, 1.5 μl of a 10 μM of four mixed dNTPs, 1.5 μl of 50 mM of MgCl2, 0.25 μl of 5u/μl Taq DNA polymerase (Cinnagene, Co., Iran) and appropriate concentrations of each primer. 1.4 μl, of IF and IR primers and 1.2 μl, of the OR and the OF primers were added to the tubes at a concentration of two picomoles (pmol), and after adding 1 μl, of template DNA, finally 3.4 μl, of Taq DNA polymerase enzyme was added. After a short vortex and then spinning the samples, the PCR steps of the desired fragments were performed using the thermal cycler: my cycler (BioRad). The amplified PCR products were checked using a primer map in the tetra-ARMS, which is shown in figure 1.
In silico analysis: In silico analyses were performed to evaluate the potential biological functions of two protomeric indel polymorphisms, rs662, located in the coding region of the PON1 gene. So, the coding sequence of the PON1 gene was screened by Polyphen-2, I-Mutant, Panther, PhD-SNP, SNP&GO, and PROVEAN prediction tools.
Statistical analysis: The Hardy-Weinberg equilibrium (HWE) was calculated for groups. All data were analyzed using SPSS software version 16. Differences in the frequency of alleles and genotypes were analyzed using the chi-square test or Fisher’s exact test. The association between PON1 gene polymorphisms and male infertility was estimated by computing the Odds Ratio (OR) and 95% Confidence Intervals (CI) from a logistic regression analysis model after adjustment for age. The p<0.05 was considered statistically significant.
Results :
Extraction of the human genome from blood was done by salting out method and to check the quality of extracted DNA, it was run on the agarose gel. Also, the concentration of samples was measured by the spectrophotometric method. Polymorphism genotyping was done by tetra-ARMS PCR method. The desired PCR product used four inner and outer primers was run on a 2% gel with an optimal binding temperature of 57.8°C. The 317 bp band is the result of two Outer primers, which can be seen in all samples. The bp band 197 bp is specific to the T allele, which is the wild allele, and the 174 bp band is specific to the C allele, which is the mutant allele. A heterozygous individual has all three bands. The wild allele homozygous individual has two 317 bp and 197 bp bands and the mutant allele homozygous individual has two 317 bp and 174 bp bands (Figure 1).
The analysis of allele frequency distribution of rs662 T>C showed that the frequency of CC, TT, and CT genotypes in healthy groups is 31, 47, and 22%, respectively. The frequency of CC, TT, and CT genotypes in the diabetic group without retinopathy was 30, 49, and 21%, respectively. Moreover, the frequency of CC, TT, and CT genotypes in the DR group was 17, 21, and 62%, respectively (Table 2).
Investigations of the SIFT database, which examines protein function when another amino acid is substituted, indicated that Q192R may affect the protein which requires further investigation. The results of the GO & SNP database showed that Q192R polymorphism is a neutral polymorphism. The Mutant-I database determines protein stability based on energy changes released by amino acid substitutions. According to the result of this database, which reported 88.0:-DDG, replacing the amino acid arginine instead of glutamine at position 129, causes a significant decrease in protein stability. This neutral polymorphism was also reported in the PROVEAN database. However, considering that the Polyphen database examined the changes caused by replacing the amino acid arginine instead of glutamine at position 129 on the protein, it does not consider these changes dangerous and has introduced this polymorphism as benign (Table 3).
Discussion :
In this study, the relationship between rs662 polymorphism and DR was evaluated in the population of Qom. The results of our study showed that there was a significant relationship between rs662 polymorphism and diabetic retinopathy in the Qom’s population. Our finding showed a significant relationship between CT allele and DR. According to our findings, there was no study on the relationship between rs662 polymorphism and DR. DR is the most severe diabetic microvascular complication. Therefore, in line with the results, some studies showed the relationship between polymorphism and vascular diseases. The immunohistochemical analysis in a study indicated that gene expression of PON1 was decreased in atherosclerotic arteries compared to normal arteries. There was a significant relationship between PON1 Q192R (rs662) polymorphism and the risk of Coronary Artery Disease (CAD). Moreover, 192R allele carriers had a higher risk of CAD compared with other allele carriers 13. Deng et al reported that rs662 (G>A) was markedly associated with Congenital Heart Defects (CHD) susceptibility compared with healthy subjects. In addition, a G allele was related to an increased risk of CHD 14. Another study demonstrated that C and R alleles were associated with T2DM susceptibility. In addition, the frequency of CC and RR genotype was markedly higher in patients with T2DM compared with healthy subjects. Moreover, CC and RR genotypes were associated with low HDL and higher LDL levels 15. GG genotype of PON1 rs662 was related to an increased risk of CAD in an Indian population. In addition, a higher frequency of the G allele was also observed in CAD patients compared with control subjects 16. However, a study reported that there was no association between PON1 (rs662) polymorphisms and diabetic dyslipidemia 17. The relationship between the PON1 rs662 polymorphism and CHD may be mediated by abnormal Ox-LDL and lipid levels caused by the R allele 18. The inconsistent findings in the relationship between Q192R polymorphism with the increased risk of vascular impairment may be due to variations in genotyping methods, sample size, pathological states, and diverse environmental effects.
Oxidative stress plays an important role in chronic inflammatory diseases such as CAD, diabetes, and DR. PON1 has a protective function due to its anti-inflammatory and antioxidant role in the body 19, 20. PON1 is mainly synthesized in liver. It is associated with HDL. Decreased PON1 levels lead to increasing ox-LDL in blood, thereby increasing the susceptibility to vascular dysfunction 21,22. PON1 rs662 gene polymorphism is involved in modulating the PON1 enzyme 23. The R allele variant is implicated in the less active isoform of PON1 against lipoprotein oxidation, and higher ox-LDL, triglycerides, and LDL-C, which lead to an increased risk of vascular dysfunction 24,25. Moreover, the inter-relationship between the PON1 and PON2 genes may affect glycaemic control in patients with diabetic retinopathy 26.
The analysis of bioinformatics software showed that this polymorphism causes a large decrease in protein stability. This decrease in stability by affecting the function of the PON1 enzyme can be a factor for the lack of hydrolysis of organophosphates. PON1 enzyme has an antioxidant role. Since the high level of Reactive Oxygen Species (ROS) plays a role in the pathogenesis of various diseases such as diabetes and heart failure and causes the destruction of the retinal capillaries and hippocampus, this factor can be a reason for the development of DR. The limitation of our study can be the relatively small sample size.
Conclusion :
The findings of this research showed that there is a significant relationship between the mutant C allele in three groups: healthy, diabetic without retinopathy, and DR causing such a result in this research. Therefore, larger population in the future research are recommended to conduct such a study.
Acknowledgement :
We appreciate all the colleagues who have worked with us in this study. We would like to extend our thanks to the University of Mazandaran (Iran) for the financial support, dedicated to the MSc candidate of Fateme Sabbaghian Bidgoli (#IranDoc1602456). Thanks to our colleagues: Mr. Mohammadkazem Heydari & Ms. Zahra Shirzad (from the Molecular and Cell biology lab, University of Mazandaran).
Conflict of Interest :
There is no conflict of interest to declare

Figure 1. Different genotypes in tetra-ARMS PCR method. A) Primer map in the tetra-ARMS PCR; B) Electrophorese patterns of genotypes in 2% agarose gel; C) Electropherograms of flanking nucleotides in the three loci.
|
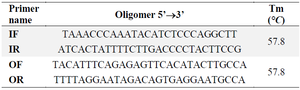
Table 1. PCR primer sequences of PON1-rs662 locus
|
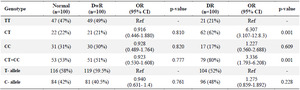
Table 2. Genotypic and allelic frequency of PON1 gene in C>T rs662 region for healthy and diseased groups
OR: Odds Ratio, CI: Confidence Interval, DwR: Diabetic without retinopathy, DR: Diabetic retinopathy.
|

Table 3. Results from bioinformatics servers
|
|