The Role of Dihydropyrimidine Dehydrogenase and Thymidylate Synthase Polymorphisms in Fluoropyrimidine-Based Cancer Chemotherapy in an Iranian Population
-
Abbasian, Mohammad Hadi
-
Department of Medical Biotechnology, National Institute of Genetic Engineering and Biotechnology (NIGEB), Tehran, Iran
-
Ansarinejad, Nafiseh
-
Department of Hematology and Oncology, Hazrat Rasool-e Akram Hospital, Iran University of Medical Sciences, Tehran, Iran
-
Cancer Pharmacogenetics Research Group (CPGRG), Iran University of Medical Sciences, Tehran, Iran
-
Abbasi, Bahareh
-
Cancer Pharmacogenetics Research Group (CPGRG), Iran University of Medical Sciences, Tehran, Iran
-
Department of Medical Genetic, Medical Biotechnology Ins., National Institute of Genetic Engineering and Biotechnology (NIGEB), Tehran, Iran
-
Iravani, Masoud
-
Tehran Gastroenterology and Hepatology Center, Tehran, Iran
-
Ramim, Tayeb
-
Department of Medicine, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran
-
Hamedi, Fahime
-
Department of Cell and Molecular Biology, Faculty of Biological Sciences, Kharazmi University, Tehran, Iran
-
 M. Ardekani, Ali
Department of Medical Biotechnology, National Institute of Genetic Engineering and Biotechnology, Tehran, Iran, Tel: +98 21 44787301; E-mail: Iranhealth@hotmail.com
M. Ardekani, Ali
Department of Medical Biotechnology, National Institute of Genetic Engineering and Biotechnology, Tehran, Iran, Tel: +98 21 44787301; E-mail: Iranhealth@hotmail.com
Abstract: Background: The fluoropyrimidine drug 5-Fluorouracil (5-FU) and the prodrug capecitabine have been extensively used for treatment of many types of cancer including colorectal, gastric, head and neck. Approximately, 10 to 25% of patients suffer from severe fluoropyrimidine-induced toxicity. This may lead to dose reduction and treatment discontinuation. Pharmacogenetics research could be useful for the identification of predictive markers in chemotherapy treatment. The aim of the study was to investigate the role of five genetic polymorphisms within two genes (DPYD, TYMS) in toxicity and efficacy of fluoropyrimidine-based chemotherapy.
Methods: Total genomic DNA was extracted from 83 cancer patients treated with fluoropyrimidine-based chemotherapy. In this study, three polymorphisms were genotyped in dihydropyrimidine dehydrogenase gene c.1905+1 G>A (DPYD*2A; rs3918290), c.1679 T>G (I560S; DPYD*13; rs55886062), and c.2846A>T (D949V; rs67376798) and two polymorphisms, besides the Variable Number of Tandem Repeat (VNTR) polymorphism and 6-bp insertion/deletion polymorphism in thymidylate synthase gene. The analysis of polymorphisms for rs3918290, rs55886062, rs67376798 and 6-bp insertion/deletion in TYMS was done by Polymerase Chain Reaction-restriction Fragment Length Polymorphism (PCR-RFLP) TYMS VNTR analysis. 5-FU-related toxicities such as anemia, febrile neutropenia, neurotoxicity, vomiting, nausea, and mucositis were evaluated according to NCI-CTC criteria version 4.0. T-test and chi-square were used and p-values less than 0.05 were considered statistically significant.
Results: DPYD gene polymorphisms were not observed in this study. The frequency of the TYMS +6 bp allele was 40.35% and the -6 bp allele was 59.65% in this study. The frequency of VNTR 2R allele was 48.75% and 3R allele was 51.15%. Toxicity grade II diarrhea, mucositis, nausea, vomiting, and neurotoxicity was 2.2, 24.1, 15.7, 6, and 51.8%, respectively. Thymidylate synthase ins/del polymorphisms were associated with increased grade III neurotoxicity (p=0.02). Furthermore, anemia grade III was significantly associated with 2R/2R genotype (0.009).
Conclusion: Thymidylate synthase gene polymorphisms may play a key role in fluoropyrimidne -based chemotherapy. Although rare DPYD polymorphisms were not observed in our study, according to large population studies, DPYD gene polymorphisms could be used as a predictive biomarker for patient treatments.
Introduction :
The fluoropyrimidine drug 5-Fluorouracil (5-FU) and the prodrug capecitabine are used for treatment of
a variety of solid cancers including gastrointestinal tract and breast 1.
5-FU/leucovorin combined with oxaliplatin (FOLFOX) is currently a standard chemotherapy regimen in treating colorectal and gastric cancers and has been shown clearly to improve response to treatment 2,3. However, the development of gastrointestinal, hematological and neurological toxicities is a major clinical problem following FOLFOX treatment 4. The clinical utility of DPYD polymorphisms has been demonstrated in a panel of markers to predict clinically actionable 5-FU toxicity. Other polymorphisms have been suggested as markers in TYMS, Enolase Superfamily Member 1 (ENOSF1) 5, MethyleneTetraHydroFolate Reductase (MTHFR) 6, ATP-binding cassette sub-family B member 1 (ABCB1) 7, and Cytidine Deaminase (CDA) 8.
Approximately, 85% of administered 5-FU dose is degraded via dihydropyrimidine dehydrogenase (DPD, encoded by the DPYD gene) 9. Functional Single-Nucleotide Polymorphisms (SNPs) in the DPYD gene alter DPD activity which may lead to the development of severe 5-FU related toxicities. The clinically most relevant variant is DPYD*2A (c.1905+1G>A, previously named IVS14+1G>A or DPD*2A), or rs3918290 10-13; DPYD*13 (c.1679T>G (rs55886062) and c.2846A>T (rs67376798) also result in low DPD activity and/or 5-fluorouracil toxicity 12-17.
A Variable Number of 28 bp Tandem Repeat (VNTR) within the promoter enhancer region (TSER) of TYMS (Thymidylate Synthase gene) is usually presented as a double-tandem repeat (2R) or a triple-tandem repeat (3R) 18-20. Second polymorphism is a 6-bp insertion/deletion in the 3ʹ-untranslated region (3ʹ-UTR) of TYMS 21. These two polymorphisms have been associated with altered TYMS expression, toxicity and an improved clinical response 13,22,23.
The aim of this study was to determine whether the five genetic polymorphisms within two genes (DPYD, TYMS) are associated with severe toxicity in patients with cancer receiving fluoropyrimidine-based chemotherapy.
Materials and Methods :
Patients and study design: Eighty three cancer patients received 5-FU-based chemotherapy at Hazrat-e Rasool hospital and Masoud clinic, Tehran, Iran between February 2014 and June 2016. The cancer types among the patients were distributed as follows: 28 colon (33.7%), 37 rectum and rectosigmoid (44.5%), and 18 stomach (21.6%). Patients were questioned about nausea and vomiting, mucositis, diarrhea, hand-foot syndrome, and neutropenia at every cycle. Eligible patients were treated with FOLFOX4 (Oxaliplatin 85 mg/m2 (2 hr infusion on day 1), leucovorin (100 mg/m2 as 2 hr infusion on day 1), 5- fluorouracil bolus (400 mg/m2) and 22 hr infusion (600 mg/m2) on days 1 and 2 every 2 weeks for 6 months (12 cycles). Toxicity was evaluated according to Common Terminology Criteria for Adverse Events (CTCAE), version 4 24. Neurotoxicity was evaluated according to the oxaliplatin-specific scale. The study was approved by the ethics committees (NIGEB) (940101-IV-503). All patients signed a written informed consent before entering the study.
Genotyping: Total genomic DNA was extracted from 200 µl whole blood using the GeneAll® kit (South Korea) and stored at -20°C until genotyping. The TYMS VNTR polymorphism was amplified by polymerase chain reaction with Taq DNA Polymerase 2×Master Mix RED (Amplicon, Denmark). Other polymorphisms were performed using a PCR–RFLP technique. RFLP analysis was performed with fast digest enzymes (Thermo Fisher Scientific, the USA). After restriction enzyme analysis, PCR fragments were visualized in a 2.5-3% agarose gel. The information of studied genetic variants is shown in table 1.
Statistical analysis: Statistical analysis was done by SPSS software version 21. The quantitative analysis was performed by descriptive variables. T-test was used for comparison of different groups and chi-square was used for qualitative analysis. p-value less than 0.05 was considered statistically significant.
Results :
Genotyping: Eighty three cancer patients (58 males, 25 females, and mean age of 57.17 years old, range of 23-86 years) were evaluated in this study. Three variants in DPYD gene were not polymorphic in this study (Table 2, Figure 1). The distribution of the rs45445694 genotype was 27.7% for 2R/2R, 30.1% for 2R/3R and 42% for 3R/3R. The distribution of the rs16430 was 38.5% for del6/del6, 42.1% for del6/ins6 and 19% for ins6/ ins6 (Table 3).
Toxicity: Toxicity data included hematological toxicities (anemia and neutropenia) in 50 patients and nonhematologic toxicities (nausea, vomiting, diarrhea, mucositis, neurotoxicity) in 83 patients. In this study, 20% (17/83) developed non-hematological grade III-IV toxicity and 29% (13/44) developed hematological grade III-IV toxicity. Anemia (18%) was the most common severe hematological toxicity, whereas mucositis (3%) and neurotoxicity (2%) were the most frequent non-hematological severe toxicities. Also, 68% of patients experienced neurotoxicity as the most severe toxicity of any grade developed during the treatment. Thymidylate synthase ins/del polymorphisms were significantly associated with increased grade III neurotoxicity (p=0.02). Anemia grade III was significantly associated with 2R/2R genotype (0.009) (Table 4).
Discussion :
Colorectal cancer is the second most common cancer in women and the third most common cancer in men worldwide 31. Colorectal cancer incidence is increasing in Iran, China and South Korea 32,33. Fluorouracil in combination with leucovorin, and oxaliplatin (FOLFOX) or with irinotecan (FOLFIRI) is the backbone of chemotherapy treatment for colorectal and gastric cancers 28,34,35. Gene polymorphisms are associated with cancer susceptibility and response to treatment in different types of cancer 36.
The aims of this study were to investigate the association of DPYD rare risk variants and TYMS polymorphisms and toxicity that may help predict the response to fluorouracil-based chemotherapy. These polymorphisms were evaluated in 83 colorectal and gastric cancer patients treated with FOLFOX regimen.
Dihydropyrimidine Dehydrogenase (DPD) is responsible for conversion of 5-FU to 5-fluorodihydro-uracil (5-FUH2) and plays a key role in the catabolism of 5-FU. Deficiency in DPD activity leads to severe toxicity which may lead to treatment discontinuation or even death. Three DPYD variants of rs3918290, rs55886062 and rs67376798 were associated with decreased DPD enzyme activity and a high risk of severe 5-FU toxicity 5,37-39. The development of severe toxicity results in dose reduction, discontinuation of treatment or even death in cancer patients 40-43.
Regarding the low minor allele frequency of the DPYD rare risk variants, three DPYD variants of rs3918290, rs55886062 and rs67376798 were not identified in the study group. This finding is consistent with some small studies 26. Similar to our study, rs3918290 polymorphism was not found in Korean, Taiwanese, Turkish, Caucasian, and African populations 44-47. In some large studies, heterozygous patients for the rs3918290 experienced severe toxicity 23,48. Some reported toxicity in just 46% of patients with rs3918290 polymorphism 13. For the rs67376798 variant, previous studies reported that 75% of patients with a heterozygous genotype experienced severe toxicity in the first two cycles of therapy 23. Other studies showed 60% or 62% of heterozygous patients experiencing toxicity within the first two cycles 13,48. The single patient with a heterozygous rs55886062 genotype experienced late toxicity after cycle 2. Loganayagam et al reported, in the largest study to date, the incidence of grade ≥3 5FU-toxicities in rs3918290, rs55886062, and rs67376798 carriers as 88.0, 50.0, and 81.5%, respectively, whereas incidence of grade≥3 overall toxicities was 88.0, 75.0, and 88.9%, respectively. Carrier of rs3918290, rs55886062 and rs37376798 had at least one grade IV toxicity of 64.0, 25.0 and 66.7%, respectively 10.
The Clinical Pharmacogenetics Implementation Consortium (CPIC) recommended reduction of fluoropyrimidine dosage in patients who are heterozygous for rs3918290, rs55886062 and rs67376798 variants which may prevent severe and possibly life-threatening toxicities. The use of 5-fluorouracil or capecitabine is not recommended in patients who are homozygous for rs3918290, rs55886062 and rs67376798 16.
Thymidylate synthase is a main intracellular target of the active 5-FU metabolite, FdUMP, which forms a ternary complex with TS and 5, 10-MTHF. rs3474303 as a variable number of tandem repeats (VNTR) is present in the 5ʹ-untranslated region (5ʹ-UTR) of the TS gene (TYMS). The three 28-bp repeat (3R) is associated with 3-4-fold translational efficiency, compared to two 28-bp repeat. In our study, the two 28-bp repeat and the 6-bp deletion allele frequencies of the TYMS gene were 48.75 and 59.65%, respectively. Significant associations were found between anemia grade III and 2R/2R TYMS genotype (0.009). In our study, association between polymorphism rs3474303 with toxicity is the same as other studies 13,20,29,49-51. 2R/3R or 3R/3R genotypes were significantly associated with a lower risk of toxicity. Although some studies have shown association between rs3474303 52 and toxicity, this association is likely to be small and clinical test would not be useful 5.
The 6-bp deletion in the 3'-UTR region of the TYMS gene affects TYMS mRNA expression 21. In our study, the del/del genotype in rs16430 was significantly associated with increased grade III neurotoxicity (p=0.02). Other studies have shown del/del genotype in rs16430 associated with diarrhea, neutropenia and mucositis (p=0.0123) 23. However, certain other studies have failed to show an association between a homozygous del/del genotype and severe toxicity 53,54.
TS mRNA level predicts fluoropyrimidine and raltitrexed sensitivity in gastric cancer 55. A meta-analysis has shown that response rates for fluoropyrimidine-based chemotherapy were significantly lower in gastric cancer patients with high TS expression 56. In Meulendijks et al’s study, TYMS VNTR 3 R/3 R genotype was formally associated with Objective Response Rate (ORR) 57.
Homozygous genotype rs1801159A/A was associated with response to fluorouracil-based adjuvant chemotherapy in gastric cancer patients 58. Another study revealed that gene polymorphisms of DPYD could be considered as a biomarker for prediction of gastric cancer patients survival treated with 5-fluorouracil-based adjuvant chemotherapy 59.
Conclusion :
In conclusion, an association was found between VNTR and TYMS 1494 ins/del polymorphism in TYMS gene and anemia and neurotoxicity, respectively. Due to the relatively limited sample size, DPYD rare risk variants of rs3918290, rs55886062 and rs67376798 were not identified in our study. Further investigations on larger sample size are needed to demonstrate the role of rare risk variants of DPYD gene. In addition, to achieve better biomarkers for FOLFOX chemotherapy regimen, additional variation in genes involved in metabolism of other drugs like oxaliplatin should be investigated.
Acknowledgement :
This work is supported in part by a grant BS-1394-01-05 from the Institute for Research in Fundamental Sciences (IPM), Tehran, Iran.The authors acknowledge the assistance of Kioomars Saliminejad in primer design and technical assistance of Shamila Darvishalipoor.
Conflict of Interest :
The authors declare that they have no competing interests.

Figure 1. Polymorphism analysis of dihydropyrimidine dehydrogenase (DPYD) and thymidylate synthase (TYMS) polymorphism. A) rs67376798; PCR product digested with BclI; lanes 1,3,5,7 and 9:113+23 bp (Wild type); lanes 2, 4, 6 and 8:136 bp (Undigested control); marker 100 bp (SinaClon, Tehran, Iran). B) rs55886062; PCR product digested with Bsp119I; lanes 1-10: 469+265 bp (Wild type); lanes 11:724 bp (Undigested control) marker 100 bp (Sina-Clon, Tehran, Iran). C) rs 3918290; product digested with Hpy CH4; lanes 1,3,5,7,9,11: 190+54 bp (Wild type); lanes 2,4,6,8,10,12: 244 bp (Undigested control); marker 50 bp (SinaClon, Tehran, Iran). D) rs45445694; lanes 3,9: 276 bp (2 repeat of 28 bp VNTR,2R); lanes 1,4,10: 304 bp (3 repeat of 28 bp VNTR,3R); lanes 2,5,6,7,8: 276+ 304 (2R3R); marker 50 bp (SinaClon, Tehran, Iran). E) TYMS 1494-del TTAAAG; lanes 1,2,10: 60+63 bp (6 bp deletion, del/del); lanes 7,11,12: 123 bp (6 bp insertion,ins/ins) lanes 3-6,8,9: 60+63+123 (ins/del); marker 50 bp (SinaClon, Tehran, Iran).
|

Table 1. Characteristics of studied DPYD and TYMS polymorphisms
a: Underlined capital letter labeled nucleotides show mismatch to complementary DNA.
b: F=forward; R=reverse; N=normal; M=mutant.
|
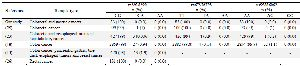
Table 2. Genotype frequencies of DPYD rs3918290, rs67376798, rs55886062 polymorphism
|
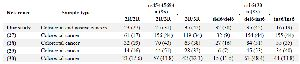
Table 3. Genotype frequencies of TYMS rs45445694 and rs16430 polymorphisms
|

Table 4. Association between TYMS polymorphisms, rs16430 and rs3474303, and toxicity after FOLFOX chemotherapy
a) Toxicity was evaluated according to Common Terminology Criteria for Adverse Events (CTCAE). Neurotoxicity was evaluated according to the oxaliplatin specific scale.
b) 50 patients were evaluable for anemia.
c) Chi-square was performed for analyzing association between TYMS polymorphisms, rs16430 and rs3474303, and toxicity. p-values less than 0.05 are statistically significant.
|
|