Leptin Receptor Gene Polymorphism may Affect Subclinical Atherosclerosis in Patients with Acromegaly
-
 Turgut, Sebahat
Pamukkale University, Medical Faculty, Department of Physiology, Denizli, Turkey, Tel: +90 258 2961698, E-mail: sturgut@pau.edu.tr
Turgut, Sebahat
Pamukkale University, Medical Faculty, Department of Physiology, Denizli, Turkey, Tel: +90 258 2961698, E-mail: sturgut@pau.edu.tr
-
Department of Physiology, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
-
Topsakal, Senay
-
Division of Endocrinology, Department of Internal Medicine, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
-
Tunç Ata, Melek
-
Department of Physiology, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
-
Herek, Duygu
-
Department of Radiology, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
-
Akın, Fulya
-
Division of Endocrinology, Department of Internal Medicine, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
-
Özkan, Şeyma
-
Department of Physiology, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
-
Turgut, Günfer
-
Department of Physiology, Faculty of Medicine, University of Pamukkale, Denizli, Turkey
Abstract: Background: Acromegaly is associated with increased morbidity and mortality related to cardiovascular diseases. Leptin (LEP) and Leptin Receptor (LEPR) gene polymorphisms can increase cardiovascular risks. The aim of this study was to investigate association between the frequencies of LEP and LEPR gene polymorphisms and subclinical atherosclerosis in acromegalic patients.
Methods: Forty-four acromegalic patients and 30 controls were admitted to study. The polymorphisms were identified by using polymerase chain reaction from peripheral blood samples. The levels of systolic and diastolic blood pressure, BMI, fasting plasma glucose, fasting insulin, IGF-I, GH, IGFBP3, leptin, triglyceride, carotid Intima Media Thickness (cIMT) and HDL and LDL cholesterol concentrations were evaluated.
Results: There was statistically significant difference between the LEPR genotypes of acromegalic patients (GG 11.4%, GA 52.3%, and AA 36.4%) and controls (GG 33.3%, GA 50%, and AA 16.7%) although their LEP genotype distribution was similar. In addition, the prevalence of the LEPR gene G and A alleles was significantly different between patients and controls. No significant difference was found among the G(-2548)A leptin genotypes of groups in terms of the clinical parameters. cIMT significantly increased homozygote LEPR GG genotype group compared to AA subjects in patients. But the other parameters were not different between LEPR genotypes groups of patients and controls.
Conclusion: It can be said that the LEPR gene polymorphism may affect cIMT in patients. The reason is that LEPR GG genotype carriers may have more risk than other genotypes in the development of subclinical atherosclerosis in acromegaly.
Introduction :
Acromegaly is a rare disease caused by excess secretion of Growth Hormone (GH) and Insulin-like Growth Factor (IGF)-I from a pituitary adenoma 1. Acromegaly is associated with increased morbidity and reduced life expectancy due to cardiovascular and cerebrovascular diseases 1,2.
Leptin is a 16 kDa protein hormone that plays a key role in regulating energy intake and energy expenditure, including appetite control and metabolism and is present in the circulation in amounts proportional to body fat mass. It is one of the most important adipose derived hormone which acts by binding and activating the long isoform of its receptor (LEPR-b) in the hypothalamus. Leptin Receptor (LEPR) has a defined novel molecular pathway for energy metabolism and regulation of body weight 3. It is worth noting that the role of leptin is supported by the universal distribution of LEPR and LEPR is selectively expressed in the central and peripheral tissues. LEPR localizes to chromosome 1p31 and the long form has 18 exons 4. LEPR, a single-transmembrane-domain receptor shows structural similarity to the class I cytokine receptor family 5. The most widely studied and most functional are the polymorphisms of G (-2548)A leptin and A668G (Q223R) leptin receptor genes 6-9.
Measurement of Intima Media Thickness (IMT) with carotid doppler Ultrasonography (USG) is a useful determiner of early atherosclerosis 8-11. However, ultrasonographic evaluation of carotid arteries showed a significant increase of IMT in patients with acromegaly only in some studies 12,13. Vitale et al demonstrated that increased levels of GH/IGF-1 were also associated with IMT increment 14. Moreover, in another study, decreases in insulin, triglyceride (TG) and fibrinogen levels together with IMT were detected as a consequence of inhibition of GH/IGF-1 secretion in acromegalic patients 12. The aim of this study was to investigate the effect of G(-2548)A leptin and A668G (Q223R) leptin gene polymorphisms on carotis IMT, plasma leptin concentrations and clinical parameters in acromegalic patients.
Materials and Methods :
Subjects: This study was performed on forty-four unrelated acromegalic patients and thirty healthy subjects. The diagnosis of acromegaly was established on the basis of criteria proposed by Freda 15. The control group consisted of 30 healthy age-matched subjects without history of chronic diseases, including cardiovascular disease, diabetes, etc. The study protocol was approved by the local Ethics Committee. The procedures were explained to all subjects and written informed consent was obtained. The study protocol conformed to the ethical guidelines of Declaration of Helsinki as reflected in a prior approval by the institution’s human research committee.
Clinical and laboratory assessment: Height and weight were measured with participants wearing light clothes and no shoes, and Body Mass Index (BMI) was calculated [(weight (kg)/height (m)2)]. Systolic and diastolic blood pressures were measured twice in the seated position after 5 min of rest. Plasma total and high-density lipoprotein cholesterol, triglycerides, GH, IGF-1, IGFBP3, Thyroid Stimulating Hormone (TSH) and insulin levels were measured.
Blood samples were obtained by vena-puncture between 8:00 AM and 10:00 AM after a requested 12 hr fast. Plasma total cholesterol, triglycerides, high density lipoprotein (HDL), light density lipoprotein (LDL), TSH, GH, IGF-1, IGFP3, insulin and glucose levels were measured immediately after vena-puncture. The serum samples were frozen at -80°C to measure serum leptin levels.
Serum leptin were measured by ELISA method with human enzyme-linked immunosorbent assay kits (Invitrogen Company, USA) according to the manufacturer’s instruction.
The cIMT measurements were made at the follow-up visit subsequent to when blood samples were obtained. B-mode ultrasonography of the left and right common and internal carotid arteries was performed by a specially trained radiology technician. Measurements were made at least 15 min after waiting and lying position. After bilateral, longitudinal and transversal examination of the carotid arteries, standardized images were obtained 2 times in 5 min intervals on each participant at 2 different points; at the lateral angle of the carotid artery bulb and 20 mm proximal of the bifurcation. The common cIMT was calculated as the mean of the left and right measurements and cIMT>0.8 was evaluated as increased thickness 16.
Genetic analysis: DNA was isolated from peripheral blood by standard phenol/chloroform extraction method. Genotyping for Leptin (LEP) gene and LEPR gene was performed by polymerase chain reaction method. PCR was performed with a thermal cycle (Techne, United Kingdom). PCR was conducted in 50 µl of a reaction mixture containing about 1 µg of DNA sample, 5 µl reaction buffer (x10) containing 160 mM (NH4)2SO4, 670 mM TrisHCL pH=8,8 0,1% Tween-20, 5 µl dNTP (2 mM), 3 µl MgCl2 (25 mM), 1 U of Platinum Taq-polymerase and 100 pmol of each of primer. The following primers were used for LEP (-2548) G→A gene polymorphism; forward 5′-TTTCCTGTAA TTTTCCCGTGAG-3′, reverse 5′-AAAGCAAAGACA GGCATAAAAA-3′.
Amplification was performed for 30 cycles, each cycle including denaturation, extension and annealing temperatures of 94oC for 45 s, 60oC for 30 s and 72oC for 1 min, respectively and the final extension time and temperature at 72oC for 10 min. The initial denaturation stage was carried out at 94oC for 2 min. The fragments obtained were electrophoresed in a 1% agarose gel and visualized by ethidium bromide staining under Ultraviolet (UV) light. PCR products were then digested by restriction enzyme Hha I at 16oC overnight. Enzyme-digested products were separated and observed through a gel imaging system.
The following primers were used for LEPR Gln223Arg gene polymorphism; forward primer 5′-ACCCTTTAAGCTGGGTGTCCCAAATAG-3′, reverse primer 5′-AGCTAGCAAATATTTTTGTAAGC AATT-3′. The PCR reaction conditions used to amplify the LEPR gene fragments were predenaturation at 94°C for 5 min, followed by thirty cycles of denaturation at 94°C for 30 s, annealing at 58°C for 30 s, and elongation at 72°C for 30 s. The last elongation at 72°C lasted for 10 min. PCR products were then digested by restriction enzyme Msp I at 16°C overnight. Enzyme-digested products were separated and observed through a gel imaging system.
Statistical analysis: Continues variables were expressed as mean± standard deviation (SD). Mann-Whitney U test was used to analyze differences in continues variables between two genotypes. Kruskal Wallis test was used to analyze differences in continues variables among three genotypes. Independent sample t test was used to analyze differences in continuous variables between two alleles groups in acromegalic patients. Chi-square test was used for comparison of nominal variables between groups. The p<0.05 were accepted as statistically significant. A correlation analysis was performed to investigate the association between the clinical parameters. All analysis was carried out using SPSS 10.0 software (Statistical Package for Social Sciences, SPSS Inc., IL, USA). Statistical significance of the observed genotype frequencies was evaluated according to Hardy-Weinberg rule compared to the expected genotype frequencies. Hardy-Weinberg equilibrium was evaluated by the χ2 test.
Results :
There were 44 patients meeting the criteria of acromegaly subjects. Clinical characteristics of patients and healthy subjects were shown in table 1. BMI, systolic and diastolic blood pressures, fasting glucose and GH, IGF-1 and IGFBP-3 levels were significantly higher in acromegalic patients compared to healthy subjects. Total cholesterol, triglyceride, HDL, LDL and leptin levels were similar between patients and controls. Also, right and left cIMTs were similar between these groups.
The frequencies of the LEP and LEPR genotype in control and acromegalic patients were shown in table 2. The frequency of the genotype LEP gene in patients showed a significant deviation from the Hardy-Weinberg equilibrium but did not show anything in controls. Observed and expected frequencies for LEP gene were in Hardy-Weinberg equilibrium in both the control group and the patients, respectively, (χ2=11.15 p<0.05), (χ2=1.6 p>0.05). The distribution of LEP genotypes in patients and control subjects were found as follows: 2 (4.5%) acromegalic patients had GG, 32 (72.7%) patients had G/A, 10 (22.7%) patients had AA genotypes, whereas in control group, 1 (3.3%) subject had GG, 15 (50%) had G/A, and 14 (46.7%) had genotypes. Regarding the frequency of genotype LEP (2548) gene, there was no significant difference between control and patients (p=0.097). The G allele was encountered in 36 (40.9%) of the patients and 17 (28.3%) of the controls. The A allele was seen in 52 (59.1%) of the acromegalic patients and 43 (71.7%) of the controls. Distribution of the alleles was not different between two groups (A/G OR=1.27; 95% CI=0.98-1.65; p=0.081).
The frequency of the genotype LEPR gene in patients and control groups did not show a significant deviation from the Hardy-Weinberg equilibrium. Observed and expected frequencies for LEPR gene were in Hardy-Weinberg equilibrium in both the patients and the controls, respectively, (χ2=0.59 p>0.05), (χ2=0.02 p>0.05). The distribution of the LEPR (223) genotype was as follows: 5 (11.4%) patients had GG, 23 (52.3%) had GA and 16 (36.4%) had AA genotype in acromegalic patients and 10 (33.3%) subjects had GG, 15 (50%) had G/A and 5 (16.7%) had AA genotype in control group (Table 2). The frequency of genotype LEPR (223) gene was significantly different between control and patients (p=0.000). The G allele was encountered in 33 (37.5%) of the patients and 35 (58.3%) of the controls. The A allele was seen in 55 (62.5%) of the acromegalic patients and 25 (41.7%) of the controls. Distribution of the alleles was significantly different between two groups (A/G OR=0.70; 95% CI=0.53-0.94; p=0.010).
The levels of systolic and diastolic blood pressure (SBP and DBP), BMI, Fasting Plasma Glucose (FPG), IGF-I, GH, IGFBP3, triglyceride, total cholesterol, HDL and LDL cholesterol, right and left cIMT and plasma leptin were compared among leptin gene genotype groups (GG, GA and AA) in patients and controls. The comparisons of characteristics among LEP gene in acromegalic patients and controls are shown in table 3.
No statistically significant difference was found among LEPR gene genotype groups (GG, GA and AA), as concerning BMI, SBP, DBP, fasting plasma glucose, IGF-I, GH, IGFBP3, triglyceride, total cholesterol, HDL and LDL cholesterol, right cIMT and plasma leptin level in patients and control individuals (Table 4). However, left cIMT in GG group was significantly higher than AA genotypes (p<0.05). In addition, the plasma IGF-1 level was significantly high in the AA genotypes of control individuals compared to GA and GG genotype subjects (p<0.05) (Table 4).
In this study, statistically significant positive correlation was found between right/left cIMT and systolic blood pressure (p<0.05). A positive correlation was observed between leptin levels and cIMT, but this was not statistically significant.
Discussion :
Acromegaly is characterized by an enhanced GH secretion. GH induces the expression and secretion of IGF-1 and high IGFBP3 level was reported in previous studies. In addition, high blood pressure and high fasting glucose were reported in acromegaly patients compared to healthy subjects. The results of the current study confirm this situation 17,18.
In this study it was revealed that there was no statistically significant difference between acromegaly and control group for LEP A2548G genotypes and alleles; however, a statistically significant difference was observed between these groups for LEPR 223 genotypes and alleles distribution in our population. LEPR 223 AA genotype and A allele frequency in acromegaly group was significantly higher than the one in control group. The LEP and LEPR gene polymorphisms were investigated for the first time in acromegalic patients. In addition, plasma leptin levels and carotid intima thickness of all subjects were determined and the relationship between these genetic and clinical parameters was investigated.
Some previous studies reported that leptin levels were low in acromegaly compared to control groups 19-21; however, other studies did not find any significant difference between patients with acromegaly and healthy subjects 22-24. In the current study, no significant differences were observed between groups, such as the second group of the study. The difference between plasma leptin levels in these studies may be due to the treatment that the patients receive or do not receive. However, Ciresi et al 25 did not compare plasma leptin levels between patients with acromegaly and healthy controls, leptin levels of newly diagnosed patients with acromegaly in their study like our results. No significant difference in leptin levels was found among LEP AA, GA, GG genotypes groups both in patients and control subjects. Also, there was no significant difference among leptin levels of LEPR gene 223 genotypes groups in acromegalic and healthy subjects. Previous studies showed a significant association of higher leptin levels with the leptin promoter polymorphism (G-2548A) 6,7,26,27 and LEPR polymorphism Q223R 8,9. However, Su et al 28 and Gaukrodger et al 29 report that there is no difference in leptin levels among the three genotypes of LEP 2548. In addition, plasma leptin levels were found similar among LEPR 223 genotypes 8,9,28. The differences between results can be attributed to these studies performed in different patient groups and different ethnic groups.
In our study, cIMT did not show significant difference between patients and controls. In addition, when the cIMT of LEP 2548 genotype individuals was analyzed within patients and the control group, no significant change was observed between genotype groups. However, when the characteristics of LEPR gene in patients and control group were compared, left cIMT significantly increased in GG genotype group vs. other genotype groups in acromegalic patients. Also, right cIMT of GG genotype subjects was greater than the other genotype groups in acromegalic patients, but the difference was not significant. The Gln223Arg genotype is associated with the lower binding capacity of leptin to the soluble form of the receptor in plasma 30. This situation causes abnormal receptor function and abnormal receptor functions lead to leptin resistance 30. It has been determined that this variant is correlated with higher BMI 31 and fat mass 30. In the current study, the BMI of patients was found higher than control subjects and it increased in GG genotype group vs. other genotypes groups in acromegalic patients. It is well known that high BMI and fat mass is a risk factor for hypertension. Increased blood pressure is a major risk factor for cardiovascular diseases. Increased blood pressure can be strongly associated with increased cIMT. Our findings seem to confirm this result. There was positive correlation between systolic blood pressure and cIMT in the current study. Accordingly, it can be said that individuals with LEPR GG genotype gene have a higher risk for high blood pressure and cardiovascular diseases.
One limitation of this study was related to the small sample size. Acromegaly is a rare disease; therefore, there is no chance to increase the number of patients. However, our study is the first one about this subject with patients having acromegaly in Turkish population. Still the findings of this study are preliminary and further studies should be carried out to confirm our results.
Conclusion :
In conclusion, the results of the present study demonstrated that acromegalic patients differ from the healthy subjects for LEPR 223 but not LEP -2548 polymorphism. In this study, only cIMTs were found to be significantly different in LEPR 223 GG genotype group compared to other genotypes within acromegalic patients. According to our data, it can be stated that the LEPR 223 GG genotype carriers may have more risk than other genotypes carriers for the development of early atherosclerosis in acromegaly. In fact, it is required to have further comprehensive studies in order to make clear this situation in acromegalic diseases.
Acknowledgement :
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Foundation project: The research is supported by The Scientific Projects Commission of the Pamukkale University (Grant number: 2011-TPF-045).
Conflict of Interest :
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
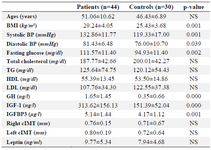
Table 1. The clinical characteristics of acromegalic patients and controls
|
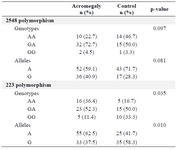
Table 2. Distribution of LEP and LEPR gene polymorphism in control and acromegalic patients
|
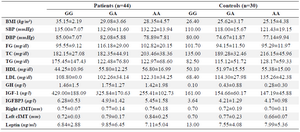
Table 3. The comparisons of characteristics among LEP gene in acromegalic patients and controls
|
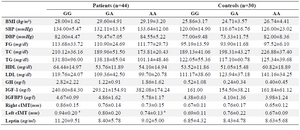
Table 4. The comparisons of characteristics among LEPR gene in acromegalic patients and controls
|
|