A Technique for Facile and Precise Transfer of Mouse Embryos
-
Sarvari, Ali
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran
-
Naderi, Mohammad Mehdi
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran
-
Sadeghi, Mohammad Reza
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, Tehran, Iran
-
 Akhondi, Mohammad Mehdi
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran , +98 21 22432020; Email: akhondi@avicenna.ac.ir
Akhondi, Mohammad Mehdi
Reproductive Biotechnology Research Center, Avicenna Research Institute, ACECR, Tehran, Iran , +98 21 22432020; Email: akhondi@avicenna.ac.ir
-
Reproductive Biotechnology Research Center, Avicenna Research Institute, Tehran, Iran
Abstract: Background: Successful Embryo Transfer (ET) technique is a fateful step of all efforts to achieve live births from in vitro produced embryos in assisted reproductive techniques or in knockout, transgenic or cloned animal projects. Small reproductive tract of mice and limitation of current techniques may not well satisfy the requirements for mass production of genetically modified mice. Genetic abnormalities of embryos, receptivity and uterine contractions, expulsion of embryos, blood, mucus or bacterial contamination on the transfer pipette tip, technical problems and even animal strain may affect embryo transfer outcome.
Methods: In this study, two techniques of embryo transfer in mice were compared. In conventional technique the oviduct wall was punctured with a 30-gauge needle and the loaded Pasteur pipette with embryos and medium was inserted into the hole. In new technique, embryos that were loaded in modified micropipette with minimal medium were transferred directly to the oviduct by manual piston micro-pump easily. Embryo viability was evaluated considering the percentage of live healthy newborns.
Results: Results of the two techniques were compared by t-test within the NPAR1WAY procedure of SAS software (ver. 9.2). The average live birth rates in the novel methods was significantly higher (42.4%) than the conventional method (21.7%, p<0.05).
Conclusion: In conclusion, using new embryo transfer technique improved birth rate by preventing embryos expulsion from the oviduct, saving time and easy transfer of embryos with minimum volume of medium.
Introduction :
Fate of all efforts to give birth to an in vitro embryo produced from infertility treatment or especially from knockout, transgenic or cloning projects depends on successful Embryo Transfer (ET) technique 1. Small reproductive tract of mouse and positive pressure in the oviduct or uterus result in the discharge of freshly transferred embryo from their point of insertion. Moreover, limitation of current equipment and techniques and the necessity of sophisticated transfer skills mainly bring about unstable pregnancy rate of genetically modified transferred embryos.
Many factors such as genetic abnormalities of embryos, defects in uterine receptivity, uterine contractions, expulsion of embryos, blood or mucus on the catheter tip, bacterial contamination of the catheter, and retained embryos have all been associated with problematic and unsuccessful embryo transfers 2. Animal strain may affect embryo transfer outcome, for example, DBA/2J mouse strain that is widely used for biomedical research suffers from poor reproductive performance 3 while F1 C57BL/6×DBA/2 (B6D2F1) and FVB/N strains are routinely used in ET programs. Heterosis, hybrid vigor, or outbreeding enhancement, is the improved or increased function of any biological quality in a hybrid offspring. Rose C. et al reported that after reciprocal embryo transfer in inbred DBA/2JHd, C3H/HeNCrl and outbred NMRI mice the highest embryo yield was achieved in outbred NMRI females, but embryo yields were similar in DBA/2J and C3H/HeN mice following superovulation de spite poor estrus cycle synchronization in DBA/2J
females 4.
The first oviduct transfer of mouse embryo was reported by Tarkowski 5, and then Whittingham demonstrated a widely-used method in rat and mouse that turned into the routine procedures for transfer of manipulated embryos 6. In conventional oviduct and uterus embryo transfer normally a puncture hole or small incision is first made in the wall of the uterus or oviduct by a 30- gauge needle for insertion of transfer pipette 7. The technique described for uterine transfer was first developed by McLaren and Mitchie 8 and extended by Rafferty 9 and Hogan 10. Various pregnancy rates ranging from 0-75% after uterine transfer have been reported 10,11. Also Michael A. et al reported a transcervical embryo transfer method in mouse using a Non-Surgical Embryo Transfer (NSET™) device 12. The recent method is suitable only for uterus embryo transfer while in some research projects oviduct transfer is needed.
To arrest transferred embryos in the oviduct or uterus, application of hyper-viscous transfer medium, placement of the embryos into the endometrium or transfer of the embryos into the uterus through the utero-tubal junction, which acts as a natural barrier, have been utilized specifically 13. Nonetheless, wide application of these modified methods has been confined by the high-skill requirements of the operating techniques. Zheng Zhang et al described a modified embryo transfer pipette with a syringe-like tip used with a mouth pipette which is the same as conventional method. They improved viability rate of mouse embryos 20% higher than conventional methods 7. In the present study, we use a modified micropipette with manual piston micro-pump that is more effective, time-saving and easy to use with minimum volume of transferred medium that eliminates the need for professional technical training.
Materials and Methods :
Preparation of modified transfer micropipette: A manual piston pump (Cell Tram oil®) (Figure 1) and micropipettes (Kwik-fil®; Borosilicate Glass Capillaries 1 mm outer diameter and 800 µm inner diameters) were used in this technique. For washing, these intact micropipettes were put in distilled water that was changed four times along 24 hr. Then put in Milli- Q water for 24 hr and were dried in oven (180-200 °C) for 1-3 hr (Figure 2A). A micropipette puller set (flaming brown, model-P97, Sutter instrument Co., USA) pulled intact micropipettes for inner diameter (I.D.) of 150-200 µm, and then by micropipete grinder EG-400 (Narishige, Tokyo, Japan) the tip was ground to a flat and diagonal opening at a 45°C angle and a sharp point (about 70-80 μm) was created at the tip by microforge MF-900 (Narishige, Tokyo, Japan) (Figure 2B).
Animals: We used eight-ten week old outbred NMRI mice for all males (fertile and vasectomised) and females (recipient and donor). They were maintained in a standard environmental and nutritional condition.
Culture of collected embryos before ET: Donors (n=10) were superovulated using i.p. injection of 5 IU HMG (Merional®: Human Menopausal Gonadotrophin, IBSA, Switzerland) and after 45-47 hr, they were received 5 IU hCG (Choriomon®: human Chorionic Gonadotropin, IBSA, Switzerland) and mated with fertile male (1:2, male: female ratio). Next day two-cell embryos were collected from donor with vaginal plug through flushing of oviduct by M2 medium. They were washed four times in M2 medium then moved to KSOM medium drops under mineral oil in 5% CO2 and 37°C incubator till ET.
Preparation of recipient mouse before ET: Recipients were mated with vasectomised males (1:2 ratio) a day after donor mating without superovulation protocol (HMG and hCG). Recipients with vaginal plugs were selected for embryo transfer. Selected recipient mice (10 recipients/group) were anesthetized with i.p. injection of ketamine (62.5 mg/kg body weight, Alfasan Co., Holland) and xylazine (6.25 mg/kg body weight, Alfasan Co., Holland). A 1 cm long skin incision was made parallel to the dorsal midline for exposing oviduct.
Oviductal embryo transfer techniques: Conventional oviductal ET: Conventional oviduct transfer was performed as control. A Pasteur pipette (outer diameter 5 mm, inner diameter approx. 4 mm, length 300 mm) was pulled on a flame smoothly to produce a tube with an internal diameter of 200-300 μm and a narrow shaft approximately 1.5-2 cm long. It loaded with a common arrangement of media (~ 10-15 μl) and three air bubbles to visualize successful transfer. The oviduct wall was punctured with a 30-gauge needle and the loaded pipette was inserted into the hole. The two-cell embryos (4 embryos/oviduct) were blown slowly into the oviduct until air bubbles became visible in the ampullae.
Novel improved oviductal ET: In this method first, two-cell stage embryos was loaded into modified embryo transfer pipette by manual piston pump (Cell Tram oil® or similar) under stereomicroscope with a common arrangement of media (≤ 1 μl) and air bubbles by a person. Then it was inserted directly into wall of the second coiled corner (counting from the ampullae) of the oviduct with the assistance of Watchmaker’s forceps under the other stereomicroscope by his colleague. First person turns the adjusting screw of pump to transfer embryo to oviduct. For evaluation of leakage and tracing the medium flow in oviduct, two control groups (10 mice/group) were selected and Trypan blue solved in M2 medium as a visible dye inserted into mice oviducts using conventional (10-15 µl) or novel (1 µl) method (Figure 3A). Oviduct was returned into the abdomen after dye injection and after some minutes it was exposed again to ensure if dye leakage occurred (Figure 3B). Embryo viability was evaluated by calculating the percentage of live healthy pup as numbers of live healthy pup divided by number of transferred embryos, in each mouse. The results of these two treatments were compared by t-test within the NPAR1WAY procedure of SAS software (ver. 9.2).
Results :
In this improved method sharp tip of modified embryo transfer pipette can be inserted easily through the wall of the oviduct, so there is no need to puncture the oviductal wall by needle before insertion of pipette. Recently, Chin and Wang performed uterine transfer from the oviduct side of the utero-tubal junction and achieved a 100% implantation rate because of their success in preventing the embryos from flowing out of the incision when they withdrew the transfer pipette 13. Using the mentioned pump equipped with a micro-adjusting screw launches a gentle, fine, fast and exact transferring instruments for oviductal ET with minimal transferred medium to the oviduct compared with conventional method (≤ 1 µl vs. 10-15 µl, respectively). Tracing inserted dye into the oviduct showed that all of the transferred embryos would remain in the oviduct lumen (Figure 3). The pregnancy rate of unmanipulated zygotes after oviduct transfer ranges from 45-80% with an average number of transferred zygotes of 25-30 14. In this study the average live birth rates in novel methods was significantly higher (42.4%) than conventional method (21.7%; Table 1; Figure 4; p<0.05). The high viability rate of transferred embryo in novel technique might be attributed to time-saving process with fewer traumas and bleeding in oviduct, effective blockage of outflow of the medium from insertion site, and less transferred medium with embryos. These results were consistent with the results of Englert et al that reported a 33.3% pregnancy rate with excellent transfer technique, whereas "bad" transfers yielded a 10.5% pregnancy rate in human 15. Similarly, Mansour et al showed that difficult embryo transfers had a significantly lower pregnancy rate and implantation rate (4 and 1%, respectively) compared with easy transfers (20.4 and 6.7%, respectively) 16. Others have reported a strong correlation between the ease of embryo transfer and pregnancy 17-19. Successful embryo transfer requires manual dexterity for introducing embryos into the reproductive tracts and preventing discharge of the transferred embryos from it; however, the latter consideration is often ignored.
Conclusion :
In conclusion, utilization of this more user friendly and less invasive tool can greatly improve the success of embryo transfer and other techniques such as spermatogonial stem cell transplantation in rete testis and so on that need fine and exact transfer instruments.
Acknowledgement :
We thank all of our friends in Avicenna Research Institute (ARI) specially our colleagues in Embryology and Animal housing departments for their good cooperation and auspices during this study.

Figure 1. Manual piston pump (Cell Tram Oil® ) used in mouse embryo transfer
|

Figure 2. A) Prepared borosilicate glass capillary; B) Sharp tip of modified embryo transfer pipette
|
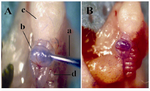
Figure 3. A) Dye injection in to oviduct by modified micropipette: modified pipette filled with trypan blue (a), second coiled ahead ampulla (b), fat pad of ovary (c), oviduct (d); B) Ampulla without leakage after dye injection
|

Figure 4. Live pup of NMRI mouse resulted from modified embryo transfer technique
|
|