Association of rs2013162 and rs2235375 Polymorphisms in IRF6 Gene with Susceptibility to Non-Syndromic Cleft Lip and Palate
-
Soleymani, Masoumeh
-
Genetics Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
-
Ebadifar, Asghar
-
Dentofacial Deformities Research Center, Research Institute of Dental Sciences, Department of Orthodontics, Faculty of Dentistry, Shahid Behehsti University of Medical Sciences, Tehran, Iran
-
Khosravi, Maryam
-
Genetics Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
-
 Khorram Khorshid, Hamid Reza
Genetics Research Center, Uni-versity of Social Welfare and Rehabilitation Sciences, Tehran, Iran, Hrkhkh1@yahoo.com
Khorram Khorshid, Hamid Reza
Genetics Research Center, Uni-versity of Social Welfare and Rehabilitation Sciences, Tehran, Iran, Hrkhkh1@yahoo.com
-
Genetics Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
-
Personalized Medicine and Genometabolomics Research Center, Hope Generation Foundation, Tehran, Iran
Abstract: Background: Non-syndromic cleft lip occurs by the interaction of environmental and genetic factors. The purpose of the current study was to analyze the association of Single Nucleotide Polymorphisms (SNPs) in IRF6 and NSCL/P in an Iranian population.
Methods: A group of 105 children with NSCL/P and 185 normal controls were included in the current study. Genotyping of IRF6 rs2013162 and rs2235375 was performed by Polymerase Chain Reaction-Restriction Fragment Length Polymorphism (PCR-RFLP) method.
Results: A substantial association of AA and CA genotypes in rs2013162 with the risk of NSCL/P (AA vs. CC; OR=2.36; 95%CI [1.05-5.29], p=0.004; and CA vs. CC; OR=0.47; 95%CI [0.28-0.79], p=0.018) was found. However, there were no important associations between A allele and risk of NSCL/P (p=0.980). According to logistic regression analysis results, subjects with GG genotype and G allele in rs2235375 polymorphism had increased risk of NSCL/P.
Conclusion: The IRF6 polymorphisms are associated with the susceptibility to NSCL/P in Iranian population.
Introduction :
Non-Syndromic Cleft Lip with or without Cleft Palate (NSCL/P) is one of the most common congenital craniofacial abnormalities which is caused by genetic factors alone or by a combination of genetic and environmental factors 1.
Contribution of genetic factors to the development of cleft lip with or without cleft palate could be proved by the fact that familial recurrence risk is higher than the risk of recurrence in general population 2. Regarding the recent advances in genotyping and sequencing methods, studies have shown a large number of Single Nucleotide Polymorphisms (SNPs) loci affecting susceptibility to NSCL/P 3. SNPs are the most common allelic variations of the genome with the frequency of more than 1% 4.
Among the susceptibility loci identified by Genome-Wide Association Studies (GWAS), the 8q24 region represents the strongest association in different populations of European ancestry, with consistent rep-lications 5. Although many susceptibility loci have been suggested by linkage and candidate gene association studies, the vast majority were non replicable across studies 6. A remarkable exception was IRF6 (interferon regulatory factor 6), in which heterozygous loss-of-function mutations lead to van der Woude syndrome and their association with NSCL/P was confirmed in several GWAS 7. The IRF6 gene on chromosome 1q32.3-q41 encodes interferon regulatory factor 6, which is a key element in oral and maxillofacial problems and is one of the candidate genes associated with both syndromic and non-syndromic forms of clefts 8. Large studies in different populations have provided the evidence that IRF6 is an important genetic factor in the etiology of NSCL/P 9. The aim of this study was to evaluate the association between the IRF6 rs2013162 and rs2235375 SNPs with the risk of NSCL/P in an Iranian population.
Materials and Methods :
Subjects
This case-control study was performed to determine the potential role of IRF6 rs2013162 and rs2235375 SNPs in developing NSCL/P in an Iranian population. A sample of 105 newborns with NSCL/P and 185 controls without cleft palate were included. A clinical examination was performed to look for dysmorphic features such as lip pits. Cases were excluded from the study if there was evidence of other facial or skeletal malformations, metabolic or neurologic disorders or anomalies of other organ systems. Samples were recruited from Mofid Hospital, a pediatric referral center in Tehran, Iran in 2013-2015. Ethical approval for the study was obtained from the ethics committee of the School of Dentistry, Shahid Beheshti University of Medical Sciences (IR.SBMU.RIDS.REC.1395.195). Informed consent was obtained from all parents in accordance with the Declaration of Helsinki 10.
Genotyping of the candidate SNPs
Genomic DNA was extracted by salting out procedure from 5 ml of peripheral blood samples. The genotyping of the subjects for IRF6 SNPs was performed by PCR and Restriction Fragment Length Polymorphism (RFLP) methods. The primer sequences and related product sizes are shown in table 1. The PCR amplification was carried out in a reaction mixture containing 10×PCR buffer, 1.5 mM MgCl2, 1 U Taq DNA polymerase (CinnaGen, Iran), 0.2 mM of dNTPs, 5 pmol of each primer, 30 ng template DNA, and sterile distilled water up to 25 µl. Amplification was performed with an initial denaturation step at 94°C for 3 min, followed by 35 cycles at 94°C for 30 s, annealing at 60°C for 40 s and extension at 72°C for 40 s, and a final extension at 72°C for 5 min. The IRF6 rs2013162 minor allele (A) was cut to two fragments of 107 bp and 67 bp, while the C allele (wild type; wt) remained uncut. In addition, the IRF6 rs2235375 minor allele (G) remained uncut, while the C allele (wt) was cut into two fragments of 137 bp and 26 bp. The PCR products of IRF6 rs2013162 and rs2235375 SNPs were digested with the restriction enzymes of DdeI and BsrBI at 37°C overnight, respectively (Figure 1). DNA fragments were subjected to 10% polyacrylamide gel electrophoresis and stained with silver nitrate. The results were confirmed by direct Sanger sequencing (Figure 2).
Statistical analysis
The Chi square (χ2) using the SPSS software V 20 (IBM, USA) was performed to compare genotype and allele frequencies in the study groups. p<0.05 were considered statistically significant.
Results :
Descriptive analysis showed that in the case group, 49.5% (52/105) and 50.5% (53/105) of the subjects were boys and girls, respectively. In the control group, 54.0% (100/185) and 46.0% (85/185) were boys and girls, respectively. The distribution of sex was not significantly different between the case and control groups (p=0.457). The genotype distribution of rs2013162 and rs2235375 polymorphisms in case and control groups was in agreement with the one predicted via Hardy–Weinberg equilibrium (HWE).
Our results showed that the frequency of the IRF6 rs2013162 CA genotype was significantly lower in the cases (36.3%) than the control (59.3%) group (p= 0.004; OR=0.47; 95% CI=0.28-0.79). On the other hand, the IRF6 rs2013162 AA (p=0.018; OR=2.36; 95% CI=1.05-5.29) was significantly higher in the NSCL/P group (14.7%) compared to the healthy children (3.3%). In addition, the IRF6 rs2235375 GG (p=0.040; OR=2.36; 95%CI=1.05-5.29) was significantly higher in the NSCL/P group (14.7%) compared to the healthy children (7.6%) and frequency of the IRF6 rs2235375 G allele in the case group (35.3%) was significantly (0.040) higher than the controls (27.0%) with the odds ratio of 1.47 (95% CI:1.02-2.13). The results are shown in tables 2 and 3.
Discussion :
In this study, the association of IRF6 common SNPs with the risk of NSCL/P in an Iranian population was evaluated. First, it was shown that the distributions of genotype in the control group for both the IRF6 rs2013162 and rs2235375 polymorphisms were in HWE. Both IRF6 SNPs, rs2013162 and rs2235375, were associated with the development of NSCL/P. This study provides additional confirmatory evidence for contribution of the IRF6 in the etiology of NSCL/P. Regarding the physiological function of IRF6, it has been shown that IRF6 was expressed in the medial edge epithelia of the fusing region of secondary palatal shelves 11. In another study, analysis of an isolated chick cDNA revealed that IRF6 levels were elevated in the epithelia covering the frontonasal process, the maxillary primordial, and nasal pits. IRF6 expression was also detected in the ectoderm of the leading edges of the developing palatal shelves and in the ridges of the primitive oral cavity 12. Bezerra et al revealed that rs2235371 in this gene is correlated with increased risk of non-syndromic orofacial clefts in Brazilian population 13. On the other hand, with sequencing of IRF6 in 100 Non-Syndromic Unilateral Cleft Lip and Palate (NSUCLP) patients, ten new and rare missense variations were identified, among which four variations were potentially deleterious 14. The common polymorphisms in IRF6 account for up to 12% of the total incidences of NSCL/P, which indicates that this gene is strongly associated with orofacial clefting 15. Huang et al found strong evidence of over- and under-transmis-sion of the rs2235375 C allele in cleft case-parent trios 16. There were significant differences in the genotype and allele frequencies of the rs2235375 in the cases and control infants 16. Analysis of five IRF6 SNPS in Mexican population revealed that the rs2235375 had the strongest association with over-transmission of the G allele with CL/P in population 17. IRF6 rs2235375 variant has also been significantly associated with increased risk of NSCL/P in co-dominant, dominant (OR=1.2), and allelic models (OR=1.4) in Indian population 18. Furthermore, a new study in Chilean population indicated that C allele of rs2235375 seems to be a risk factor for NSCL/P 19. In a recent study by Xu et al there was a significant difference in both genotypic and allelic distributions between patients and controls at rs2013162. In addition, case-parent analysis revealed over-transmission of the rs2013162A allele 20. In another Chinese population, rs2013162 showed a significant association with NSCL/P 21. However, another study on Mexican patients revealed that rs2235375 and rs2013162 in IRF6 gene were not associated with NSCL/P 22.
Conclusion :
In conclusion, the results of the current study indicated that two IRF6 SNPs, rs2235375 and rs2013162, were associated with the NSCL/P in Iranian population.
Acknowledgement :
We would like to thank the patients who participated in this study.
Conflict of Interest :
The authors declare no conflict of interest.
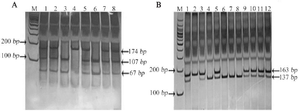
Figure 1. Representative gel pictures of polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) results. A) The rs2013162 C/A polymorphism PCR-RFLP result. Lane M; Ladder 100 bp, No. 1,2,5,7 and 8: heterozygote (CA), No. 3; homozygote (AA), No. 4; homozygote (CC), B) The rs2235375 G/A polymorphism PCR-RFLP result. Lane M; Ladder 100 bp, No. 1,3,5,9,10,11 and 12; heterozygote (CG), No. 2; homozygote (GG), No. 4,6,7 and 8; homozygote (CC).
|
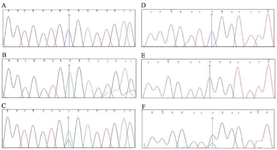
Figure 2. Sequencing results. Polymorphism rs2013162. A) CC homozygote (wild), B) AA homozygote (variant), C) CA heterozygote. Polymorphism rs2235375, D) CC homozygote (wild), E) GG homozygote (variant), F) CG heterozygote.
|

Table 1. Primer sequences used for the genotyping of the IRF6 polymorphisms
|
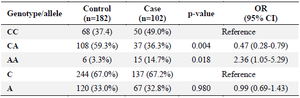
Table 2. Genotype and allele frequencies of IRF6 rs2013162 SNP in cleft lip/palate and control groups
|
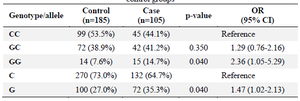
Table 3. Genotype and allele frequencies of IRF6 rs2235375 SNP in cleft lip/palate and control groups
|
|